EMG Biofeedback: Uses & Electrode Sites
Electromyographic (EMG) biofeedback (EMG BFB), approved by the U.S. Food and Drug Administration (FDA) in 1991, has been safely and effectively used with no reported side effects. As the most widely adopted biofeedback method for neurological and neuromuscular rehabilitation, surface EMG biofeedback offers a convenient and effective solution for home use. This non-invasive therapy helps patients strengthen weak or paretic muscles or reduce spastic muscle tone—all from the comfort of their own home. Thanks to its portability and user-friendly design, electromyographic biofeedback empowers patients to take an active role in their recovery, making it an ideal choice for long-term management of chronic conditions, post-stroke rehab, and mobility disorders.
In this article, you’ll find a step-by-step guide on using EMG biofeedback at home, including electrode placement (with visual location guides), optimal usage timing, troubleshooting tips, and more, ensuring you maximize its benefits safely and effectively.
Table of Contents
ToggleElectromyography (EMG) is an instrument that records the electrical activity of the muscles. It is a diagnostic procedure to assess the health of muscles, the nerve cells that control them, and the conducting function of nerves.
When muscles become active, they produce an electrical current. In fact, this current is typically proportional to the level of muscle activity. Specifically, the EMG (electromyography) signal is a biomedical signal that measures electrical currents generated during muscle contraction, effectively representing neuromuscular activity. However, various factors, including muscle physiology, temperature, cross-sectional area, and muscle length, can significantly influence EMG signal recordings.
Electromyographic EMG biofeedback measures and transforms the physiological information from muscle into visual and audio signals. It can increase activity in weak or paretic muscles or facilitate a reduction in tone in spastic ones.
EMG Biofeedback Loop
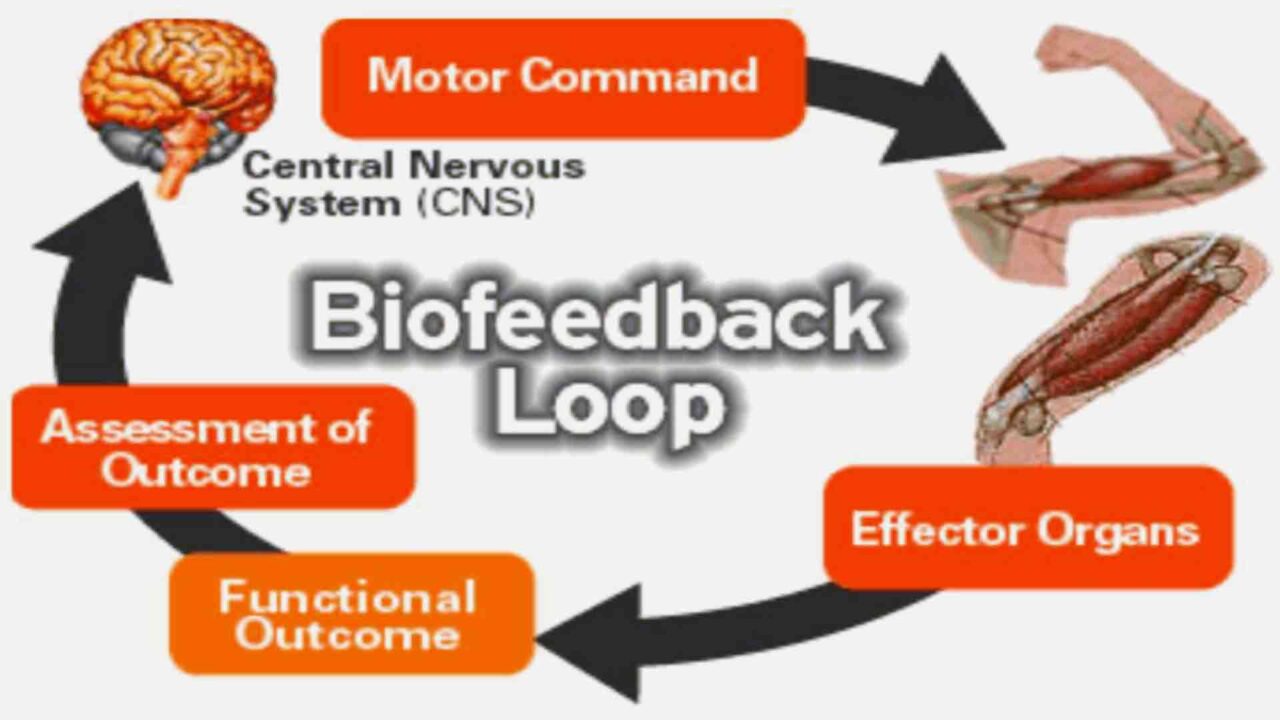
During an injury, not only are bones, ligaments, and muscles hurt, but special nerve receptors are also hurt. These receptors in muscles send information back to the brain about where the body’s joints are while in motion and how hard they are working. Injury is much more likely to reoccur if these receptors are not retrained during rehabilitation. It has been shown that electromyographic EMG biofeedback is helpful in both musculoskeletal and neurological rehabilitation.
Indications for Ectromyographic EMG Biofeedback Use
Electromyographic EMG biofeedback used
- to facilitate muscle contractions,
- to promote increased motor recruitment and improve poor mechanics,
- to regain neuromuscular control,
- to retrain joints’ function after injury,
- to improve posture,
- to improve gait patterns,
- to improve balance
- to decrease muscle spasms,
- to calm down overactive muscles,
- to promote relaxation
Electromyographic biofeedback devices use surface electrodes to detect electrical activity in skeletal muscle. They can be used in one of two ways:
- To retrain injured muscles
- To calm down overactive muscles
Skin Preparation and Electrode Placement Sites for Surface EMG Biofeedback
Proper skin preparation
Proper skin preparation and surface EMG biofeedback electrode positioning are essential for acquiring quality EMG measurements.
While there are no general rules for skin preparations, the type of application and signal quality usually determine the extent of skin preparation. For example, given a targeted test condition, if the movement is somewhat static or slow-moving and only qualitative reading is desired, a simple alcohol swab around the area of interest is sufficient. However, if dynamic conditions present a risk of the introduction of movement artifacts, like in walking, running, or other planned accelerated movements, thorough preparation is required. Skin preparation for surface electrodes usually involves removing the patient’s hair around the electrode site to improve electrode adhesion.
Cleaning the skin then involves one of the following methods:
For effective static EMG measurements, strict use of alcohol swabs to clean the skin surface is often sufficient. However, for more accurate results, fine sandpaper should be used to abrade the skin surface, combined with alcohol swabbing, to clean dead skin, oil, and dirt and thereby lower skin impedance. Additionally, special abrasive and conductive pastes help remove dead skin and reduce skin impedance.
Surface EMG Biofeedback Electrode Placement Sites
The recommended differential electrode placement sites for fine wire and surface EMG biofeedback are shown in the image provided. These sites are well-defined and referred to as anatomical landmark sites.
When placing the differential electrode pairs, the following guidelines should always be followed:
- First, ensure the placements are aligned with the direction of the muscle fibers under study.
- Second, electrodes should be positioned as close to the monitored muscle as possible.
- Third, place electrodes parallel to the direction of the muscle fibers.
- Finally, pay attention to the spacing of the electrodes, as this is critical for reducing extraneous electrical activity (noise).
By following these steps carefully, you can optimize the quality and accuracy of EMG readings.
When required, placement of the reference electrode is typically more proximal and away from the differential electrodes, preferably on electrically neutral tissue (say, over a bony joint).
Recommended electrode placement sites for EMG Biofeedback

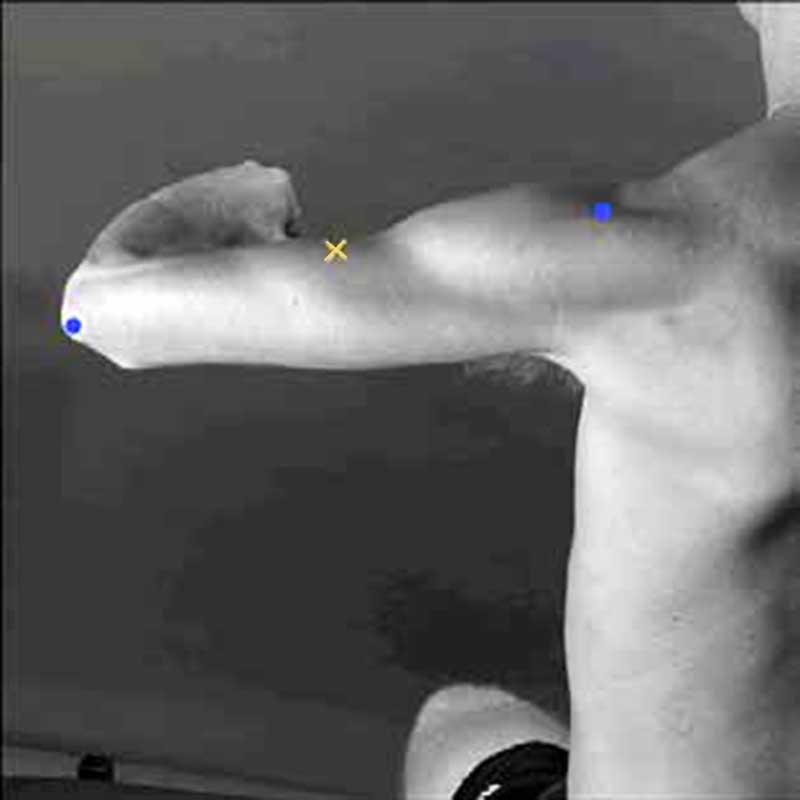
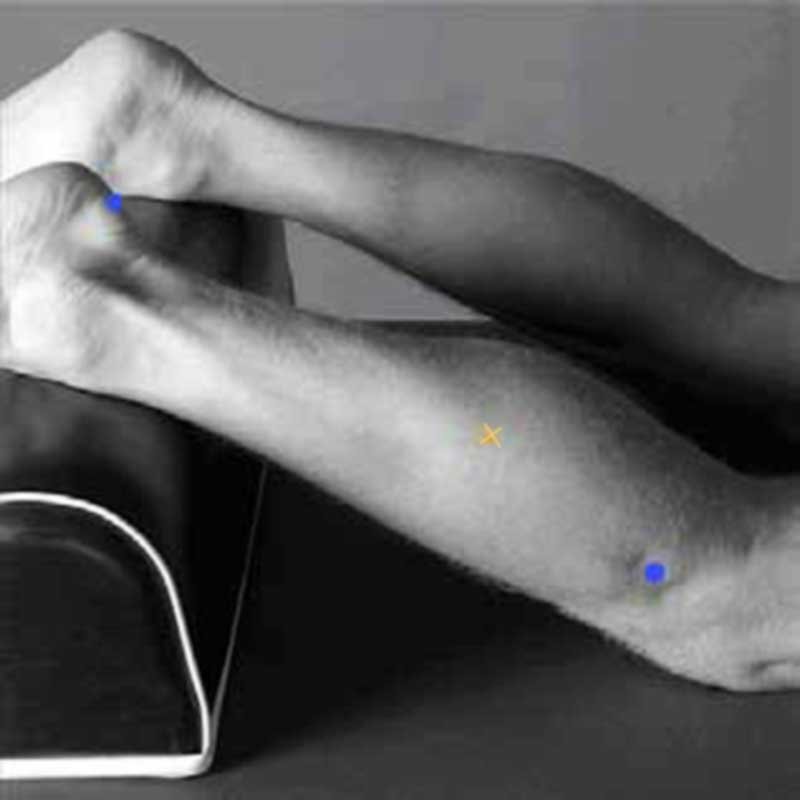
Biceps Bracchi
| Anatomy | |
| Subdivision | Short and Long head |
| Function | Elbow flexion |
| Placement | |
| Start position | Flexed elbow at a right angle, the dorsal side of the forearm in a horizontal downward position |
| Location | Line medial acromion – fossa cubit, at 1/3 from fossa cubit (elbow pit) |
| Orientation | Parallel to line acromion – fossa cubit |
| Test | Flex the elbow while applying pressure to the forearm in the direction of extension |

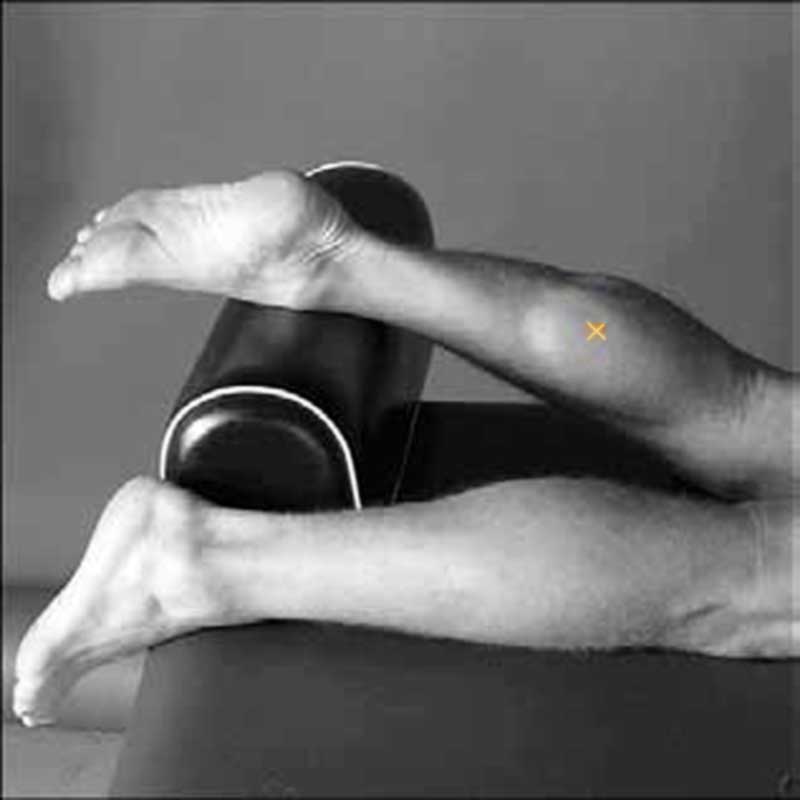
Triceps Bracchi (long head)
| Anatomy | |
| Subdivision | Long head |
| Function | Elbow extension, adduction, shoulder extension |
| Placement | |
| Start position | The shoulder at 90° abduction with the arm 90° flexed, the palm pointing downward |
| Location | At 50% of the line posterior crista of acromion–olecranon, two fingers medial to this line |
| Orientation | Parallel to line posterior crista of acromion – olecranon |
| Test | Extend the elbow while applying pressure to the forearm in the flexion direction. |

Triceps Bracchi (lateral head)
| Anatomy | |
| Subdivision | Lateral head |
| Function | Elbow extension |
| Placement | |
| Start position | The shoulder at 90° abduction with the arm 90° flexed, the palm pointing downward |
| Location | At 50% of the line posterior crista of acromion–olecranon, two fingers lateral to this line |
| Orientation | Parallel to line posterior crista of acromion – olecranon |
| Test | Extend the elbow while applying pressure to the forearm in the flexion direction. |
Rectus Femoris
| Anatomy | |
| Subdivision | |
| Function | Extension of the knee joint and flexion of the hip joint |
| Placement | |
| Start position | Sitting on the table, knees in slight flexion, upper body slightly bent backward |
| Location | At 50% of line anterior spina iliaca superior -superior part of the patella |
| Orientation | Parallel to line anterior spina iliaca superior -superior part of the patella |
| Test | Extend the knee while pressing against the leg above the ankle in the direction of flexion. |
Vastus Medialis
| Anatomy | |
| Subdivision | |
| Function | Extension of the knee joint |
| Placement | |
| Start position | Sitting on the table, knees in slight flexion, upper body slightly bent backward |
| Location | At 80% of line anterior spina iliaca superior -anterior border of the medial ligament |
| Orientation | Almost perpendicular to the line anterior spina iliaca superior – -anterior border of the medial ligament |
| Test | Extend the knee while pressing against the leg above the ankle in the direction of flexion. |
Vastus Lateralis
| Anatomy | |
| Subdivision | |
| Function | Extension of the knee joint |
| Placement | |
| Start position | Sitting on the table, knees in slight flexion, upper body slightly bent backward |
| Location | At 2/3 of line anterior spina iliaca superior – lateral side of the patella |
| Orientation | In the direction of muscle fiber |
| Test | Extend the knee while pressing against the leg above the ankle in the direction of flexion. |
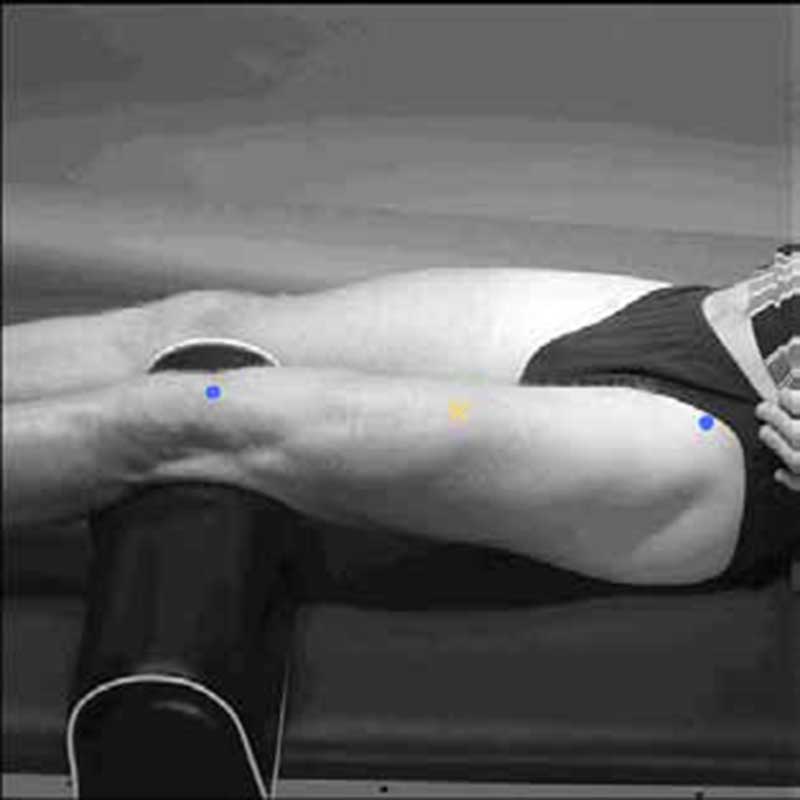
Biceps Femoris
| Anatomy | |
| Subdivision | Long head (LH) and short head |
| Function | Flexion and lateral rotation of the knee joint. LH also extends lateral rotation of the hip joint |
| Placement | |
| Start position | Lying on the belly, thigh down on the table, knees flexed, thigh in slight lateral rotation, leg in slight lateral rotation concerning the thigh |
| Location | At 50% of line ischial tuberosity – lateral epicondyle of the tibia |
| Orientation | Parallel to line ischial tuberosity – lateral epicondyle of the tibia |
| Test | Press against the leg proximal to the ankle in the direction of knee extension. |
Tibialis Anterior
| Anatomy | |
| Subdivision | |
| Function | Dorsiflexion of the ankle joint, inversion of the foot |
| Placement | |
| Start position | Supine or sitting |
| Location | At 1/3 of the line tip of the fibula – the tip of the medial malleolus |
| Orientation | Parallel to the line tip of the fibula – the tip of the medial malleolus |
| Test | Support the leg just above the ankle joint with the ankle joint in dorsiflexion and the foot in inversion without extension of the big toe. Apply pressure against the foot’s medial side and dorsal surface in the direction of plantar flexion of the ankle joint and eversion of the foot. |

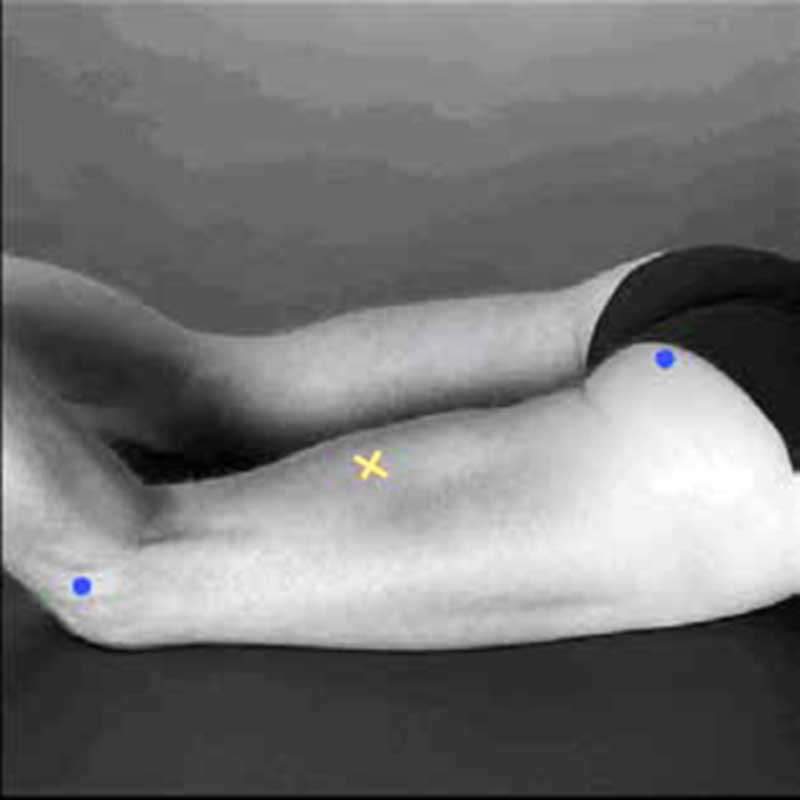
Soleus
| Anatomy | |
| Subdivision | |
| Function | Plantar flexion of ankle joint |
| Placement | |
| Start position | Sitting with knee approx. 90° flexed and heel/foot on the floor |
| Location | At 2/3 of line medial condyles of the femur – medial malleolus |
| Orientation | Parallel to line medial condyles – medial malleolus |
| Test | Put a hand on the knee and push the knee down while asking the subject to lift the heel from the floor. |

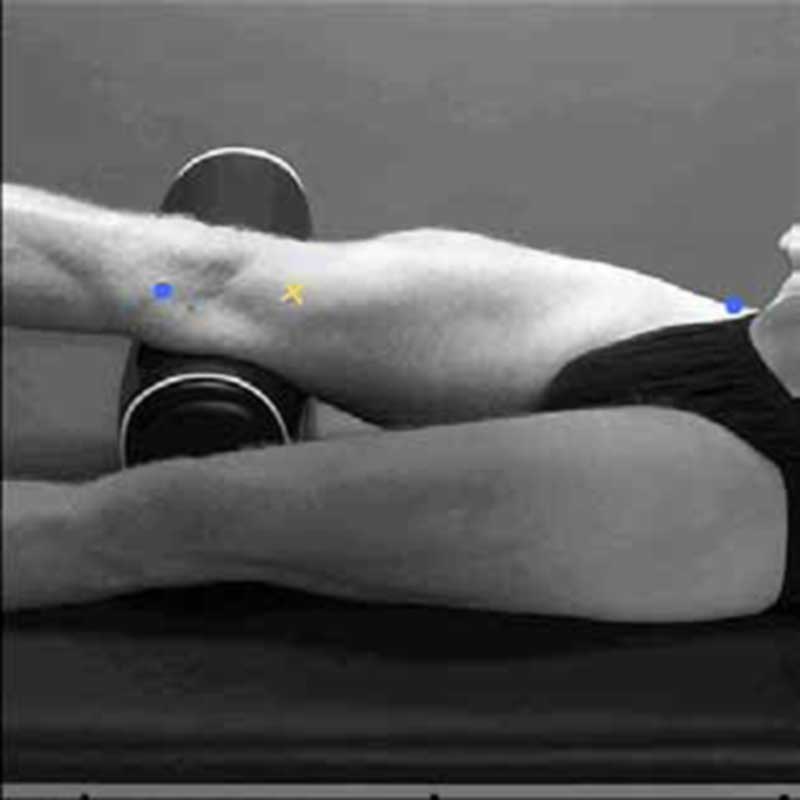
Gastrocnemius Medialis
| Anatomy | |
| Subdivision | Medialis |
| Function | Flexion of ankle joint, flexion of knee joint |
| Placement | |
| Start position | Lying on the belly, knee extended, foot projecting over the end of the table |
| Location | At the most prominent bulge of muscle |
| Orientation | Parallel to the lower leg |
| Test | Plantar flexion of the foot with an emphasis on pulling the heel upward more than pushing the forefoot down. Apply pressure against the forefoot as well as calcaneus. |
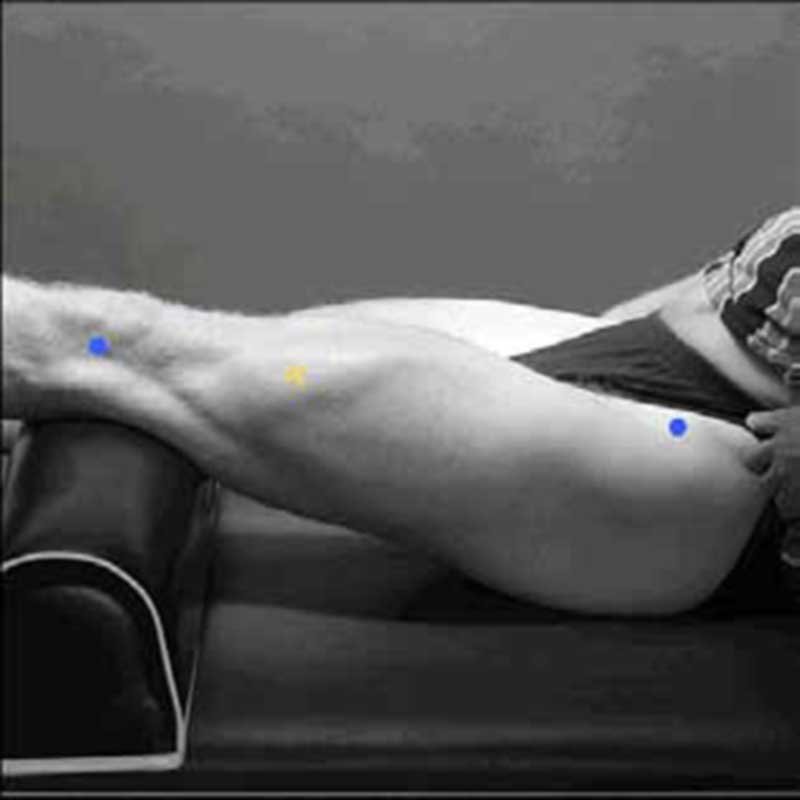
Gastrocnemius Lateralis
| Anatomy | |
| Subdivision | Lateralis |
| Function | Flexion of ankle joint, flexion of knee joint |
| Placement | |
| Start position | Lying on the belly, knee extended, foot projecting over the end of the table |
| Location | At 1/3 of the line head of fibula – heel |
| Orientation | Parallel to line head of fibula – heel |
| Test | Plantar flexion of the foot with an emphasis on pulling the heel upward more than pushing the forefoot down. Apply pressure against the forefoot as well as calcaneus. |
Applications and Benefits of Surface EMG Biofeedback
Medical
- Orthopedic
- Surgery
- Functional neurology
- Gait and posture analysis
Rehabilitation
- Post-surgery/accident
- Neurological rehabilitation
- Physical therapy
- Active training therapy
Ergonomics
- Analysis of demand
- Risk prevention
- Ergonomic design
- Product certification
Sport science
- Biomechanics
- Movement analysis
- Athletes strength training
- Sports rehabilitation
Practical medical applications of electromyographic biofeedback involve its use in pre- and post-procedural assessment and treatment. Additionally, it is used for the prevention or retardation of muscle atrophy, as well as increasing local blood circulation. Furthermore, electromyographic biofeedback aids in relaxing muscle spasms, maintaining or increasing range of motion, and muscle re-education and rehabilitation.
For stroke survivors and patients diagnosed with incontinence (the loss of voluntary control over excretory functions), structured rehabilitation programs play a crucial role in recovery. Specifically, these training regimens are designed to help individuals gradually restore functional control over affected muscle groups. Over time, through consistent practice and targeted exercises, patients typically demonstrate measurable improvements in both muscle coordination and voluntary control. Importantly, this progressive approach enables them to regain independence in daily activities previously compromised by their condition. The electrical activity during a patient’s muscle contraction and relaxation cycle is often characteristically different or much weaker and more challenging to detect at damaged muscle sites.
Electromyographic biofeedback offers both the patient and therapist objective, real-time information about the subject’s muscle activity. This is achieved by carefully and skillfully placing specific electrodes on targeted sites. As a result, the electromyographic biofeedback user benefits from immediate feedback, which significantly enhances self-awareness of muscular activity under direct conscious control. Additionally, this instant feedback accelerates the therapist’s ability to provide effective instruction, ultimately improving the patient’s capacity to perform specific movements more efficiently.
The conditions listed below can benefit from electromyographic biofeedback:
- Muscle atrophy or weakness due to disease or injury ( Stroke, Spinal cord injury, Chronic musculoskeletal injury),
- Joint contracture,
- Bruxism and TMJD
- Balance and mobility disorders,
- Trunk muscle re-education,
- Respiratory muscle control,
- Hypertension,
- Idiopathic Raynaud’s disease,
- Posture pathology, scoliosis, osteochondrosis,
- Club-foot,
- Pain,
- Cauda equina syndrome with neurogenic bladder,
- Incontinence
– Anal sphincter spasm.
– Atonic bladder,
– Extrinsic urethral sphincter deficiency,
– Urethral instability.
– Fecal incontinence,
– Specific and non-specific acute urinary retention,
– Incomplete bladder emptying,
– Urgency urinary incontinence,
– Female stress urinary incontinence,
– Female and male mixed urinary incontinence,
– Urinary incontinence without voiding desire,
– Post-micturition dribbling,
– Nocturnal enuresis,
– Continuous leakage and urinary frequency,
Contraindications for Surface EMG Biofeedback Performance
- If the patient is prohibited from moving the joint or isometric contractions, then EMG BFB should not be used,
- Unhealed tendon grafts,
- Avulsed tendon,
- A third-degree tear of muscle fibers,
- Unstable fracture,
- Injury to joint structure, ligaments, capsule, or articulating surface.
EMG Biofeedback FAQ
Electromyographic (EMG) biofeedback is a therapeutic technique that uses sensors to detect and display real-time electrical activity from your muscles. Through visual cues (like graphs or games) or auditory signals, it helps you develop awareness and control over muscle tension. This method supports rehabilitation, pain management (e.g., for migraines or chronic pain), and neuromuscular retraining. While often administered by clinicians, portable EMG devices now enable guided at-home use.
Yes! Research demonstrates that surface EMG biofeedback can effectively reduce chronic pain by teaching patients to recognize and release excessive muscle tension. Clinical studies support its use for conditions like lower back pain, fibromyalgia, sciatica, and tension headaches. By providing real-time feedback, it helps retrain muscle patterns, leading to lasting pain relief.
The optimal frequency depends on your goals:
Chronic pain management (e.g., back pain, fibromyalgia):
Daily or near-daily sessions (5–7x/week) for 15–30 minutes to reinforce muscle relaxation and reduce tension patterns.
Rehabilitation/recovery (e.g., post-injury, muscle imbalances):
3–5 sessions weekly for 10–20 minutes to monitor progress and avoid overexertion.
Athletic performance & muscle training:
2–3x weekly for 10–15 minutes—pre-workout to activate target muscles or assess tension and recovery post-workout.
Consistency matters more than session length. Start with shorter sessions and adjust based on your device’s feedback.
Absolutely! It’s proven to reduce jaw tension. Place sensors on the masseter muscle and practice relaxation techniques.
ELECTROMYOGRAPHIC BIOFEEDBACK HOME USE DEVICES
There are several types of electromyographic biofeedback devices. However, the most complex ones are usually in therapeutic and clinical settings. In these cases, a doctor or healthcare professional typically administers them so you can get the most out of the treatment.
However, there are also smaller, less powerful (but still helpful) devices that you can purchase and use as part of a daily regimen to help train your body to overcome its unconscious muscular reactions to the stress and anxiety of modern life.
The uses of electromyographic biofeedback aren’t limited to just stress and stress-related conditions. They also help those suffering from chronic migraines and assist with psychological therapies such as mindfulness meditation. Some athletes, for example, have been experimenting with electromyographic biofeedback therapies to help them achieve new heights of physical fitness. Additionally, an electromyographic EMG biofeedback home-use device can also be used to solve muscular rehab problems.
NeuroTrac® Simplex
NeuroTrac® Simplex is a single-channel EMG unit suitable for diagnosing, monitoring, and treating a wide range of muscle problems.
- Suitable for diagnosing, monitoring, and treating a wide range of muscle problems
- Single Channel EMG unit
- The optional multilingual computer database system
- Structured protocols for consistency of patient progress reports (software)
- Used as an surface EMG biofeedback training aid or diagnostic tool
- Measures EMG from 0.2µV to 2000µV Accurately
- Designed for a wide range of physiotherapy applications such as incontinence, shoulder and neck pains, patellofemoral pain, repetitive strain injury, stroke, plus much more
- Used as a learning tool for both patients and therapists with an emphasis on improving rehabilitation techniques
- Produces and prints comprehensive patient progress reports of work/rest averages, onset contraction and muscle release times, peak values, and work/rest average deviations (with optional software)
- Ability to lock the unit
- Records EMG statistics
- User-friendly
- Compact, light, and reliable
- Easy-to-use optional software available
- Low-cost, high quality and very accurate



You can easily power on this biofeedback unit, and then the real-time EMG will be continuously measured. Next, you can press the START button to begin the Work/Rest program. At this point, you will be prompted to contract and relax your muscles. When the session is finished, the statistics will be displayed on the LCD: work time, rest time, onset, and release time. One easy-to-use customizable program where you can use the default settings or change work time, rest time, number of repetitions, etc.
NeuroTrac® MyoPlus2 Pro
NeuroTrac MyoPlus2 Pro is a new and improved touch-screen with a full-color display. The new user-friendly interface makes it a self-explanatory unit with interactive learning on the go, including electrode placement, running EMG graph, as well as many other helpful tools.
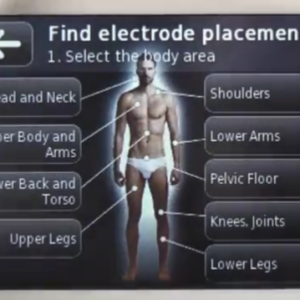
- This device features a new and improved touch screen with a full-color display. Moreover, the user-friendly interface makes it a self-explanatory unit, allowing for interactive learning on the go. For instance, it includes electrode placement guides, a running EMG graph, electromyographic EMG biofeedback games and templates, as well as many other helpful tools.
- Pre-set programs for Incontinence treatment, Sports and muscular development, and neuromuscular Rehabilitation.
- Designed for Physiotherapists as a portable tool, it is suitable as a personal trainer for in-clinic or home use (under guidance).
- Two-channel EMG (Biofeedback) combined with two channels of NMES (stimulation).
- Two-channel ETS (EMG triggered stimulation) with stimulation on two channels.
- Simple single-phase or multiphase operation: multiphase allows EMG/ETS/STIM to be combined in one program.
- Multilingual LCD screen and voice prompts for Biofeedback.
- Manual and Automatic threshold control.
- EMG Biofeedback between stimulation (muscle activity and tiredness indication when using muscle stimulation).
- Stand-alone device or used in conjunction with established multilingual software.
- Up to 10 meters of wireless (Bluetooth) connection for NeuroTrac Software.
- For home users, this device effectively produces and prints comprehensive patient progress reports daily using the optional PC software. These reports provide average readings from two channels, including work/rest times, peak and onset times, muscle release times, work and rest deviations, and the average mA current.
- Used as a learning tool for both patient and clinician with emphasis on improving treatment techniques in the use of EMG and Neuromuscular stimulation.Model number: MYO220P. This product is available through selected distributors who can provide training and support.