Do you ever feel like your brain is not performing at its best? You are not alone—millions of people struggle with mental focus, memory retention, and learning efficiency every single day. The good news is that your brain health is not fixed, and you can actively train your neural networks for peak cognitive performance. Neurofeedback is a science-backed approach that uses real-time brainwave monitoring to help you improve cognitive performance. Whether you want to improve brain function and memory, increase brain function for work or study, or improve attention and focus for daily tasks, neurofeedback offers a proven solution. The BrainBit family of neurofeedback devices is designed to help you improve cognitive performance and enhance your learning ability. This guide will show you how to choose the right device for your unique goals. Since different brain regions control different functions, match your needs to the correct electrode coverage.
To maximize cognitive performance, targeted neurofeedback training must address the specific cortical networks governing each mental faculty:
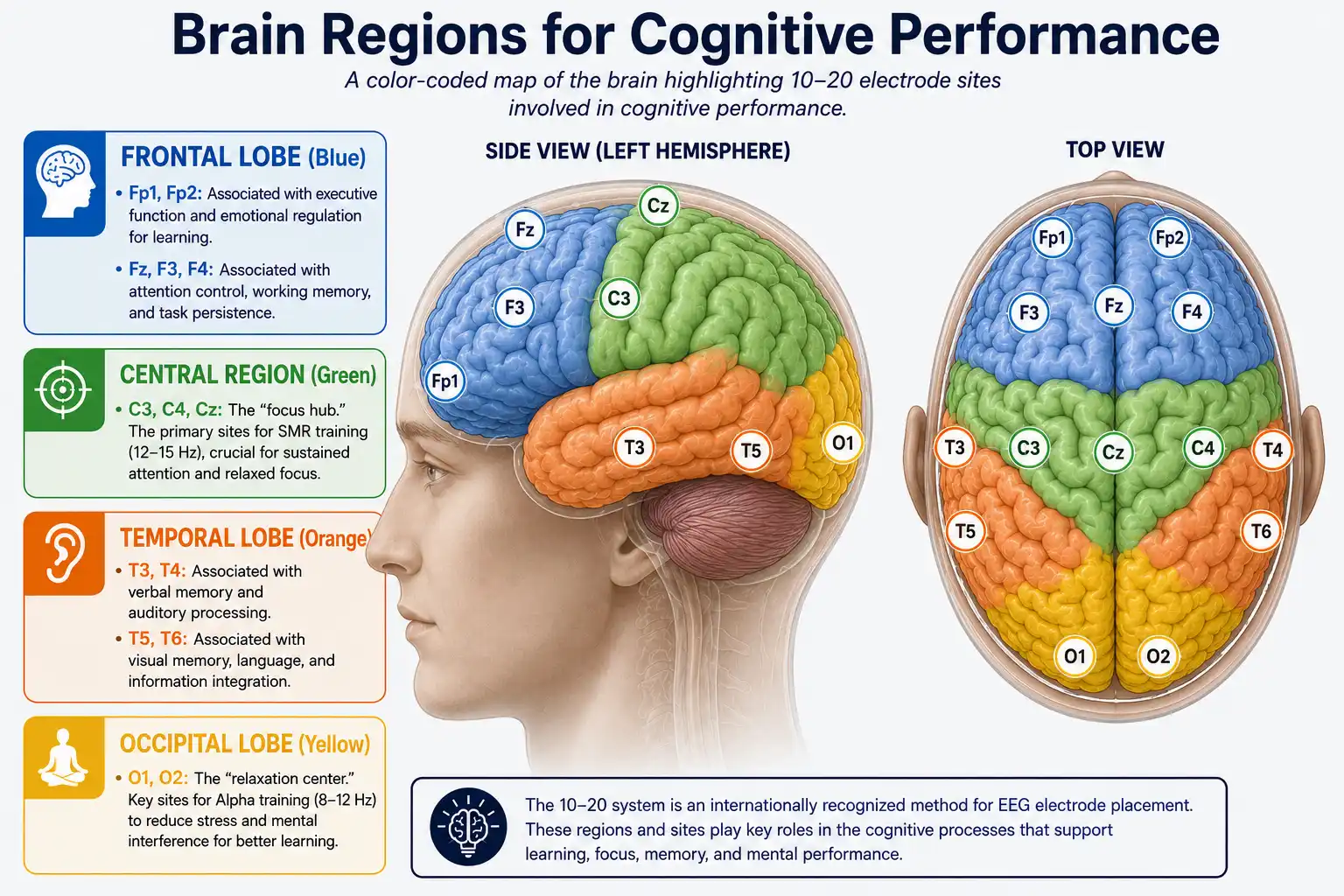
- Attention and Focus: Trained via central sites (C3, C4, Cz) and frontal sites (Fp1, Fp2, Fz) using SMR up-training or Theta/Beta protocols.
- Verbal Memory: Enhanced through temporal sites (T3, T4) utilizing Theta up-training and Alpha-Theta protocols.
- Visual Memory: Optimized at posterior temporal sites (T5, T6) via Low-Beta enhancement protocols.
- Learning Efficiency: Supported by combining all the above regions with occipital sites (O1, O2) using Alpha relaxation and SMR/Theta ratio training.
The BrainBit family provides EEG headbands with different electrode configurations to target these specific brain regions and protocols.
How to Improve Cognitive Performance with Neurofeedback
Have you ever read a page and absorbed nothing? Or sat down to study, only to drift off within minutes? Do you forget names, facts, or where you put your keys? Does learning new skills feel harder than it should?
You are not alone. In fact, millions face these challenges daily. However, these are not signs of a failing brain. Instead, they signal that your brain needs the right training.
This is where neurofeedback comes in.
Neurofeedback is a science-backed approach that uses real-time brainwave monitoring to train specific cognitive functions. By targeting brain regions responsible for attention, memory, and learning, you can gradually improve mental performance.
But here is the key: different cognitive functions reside in distinct brain regions. Therefore, to improve a specific function, you need electrodes positioned over the correct region.
This guide will help you understand:
- Which brain regions control attention, focus, memory, and learning efficiency
- Which neurofeedback protocols are proven to enhance each function
- Which BrainBit device is best for your specific cognitive goals
What Is Cognitive Performance?
Cognitive performance determines how effectively your brain processes information, sustains attention, stores and retrieves memories, and acquires new knowledge. Therefore, it underpins everything you do—from work and studies to daily life.
The four pillars of cognitive performance are:
| Pillar | What It Does |
|---|---|
Attention |
The ability to select and focus on relevant information while ignoring distractions |
Concentration/Focus |
The ability to sustain that attention over time without mental fatigue |
Memory |
The ability to encode, store, and retrieve information |
Learning Efficiency |
The ability to acquire new skills and knowledge quickly and effectively |
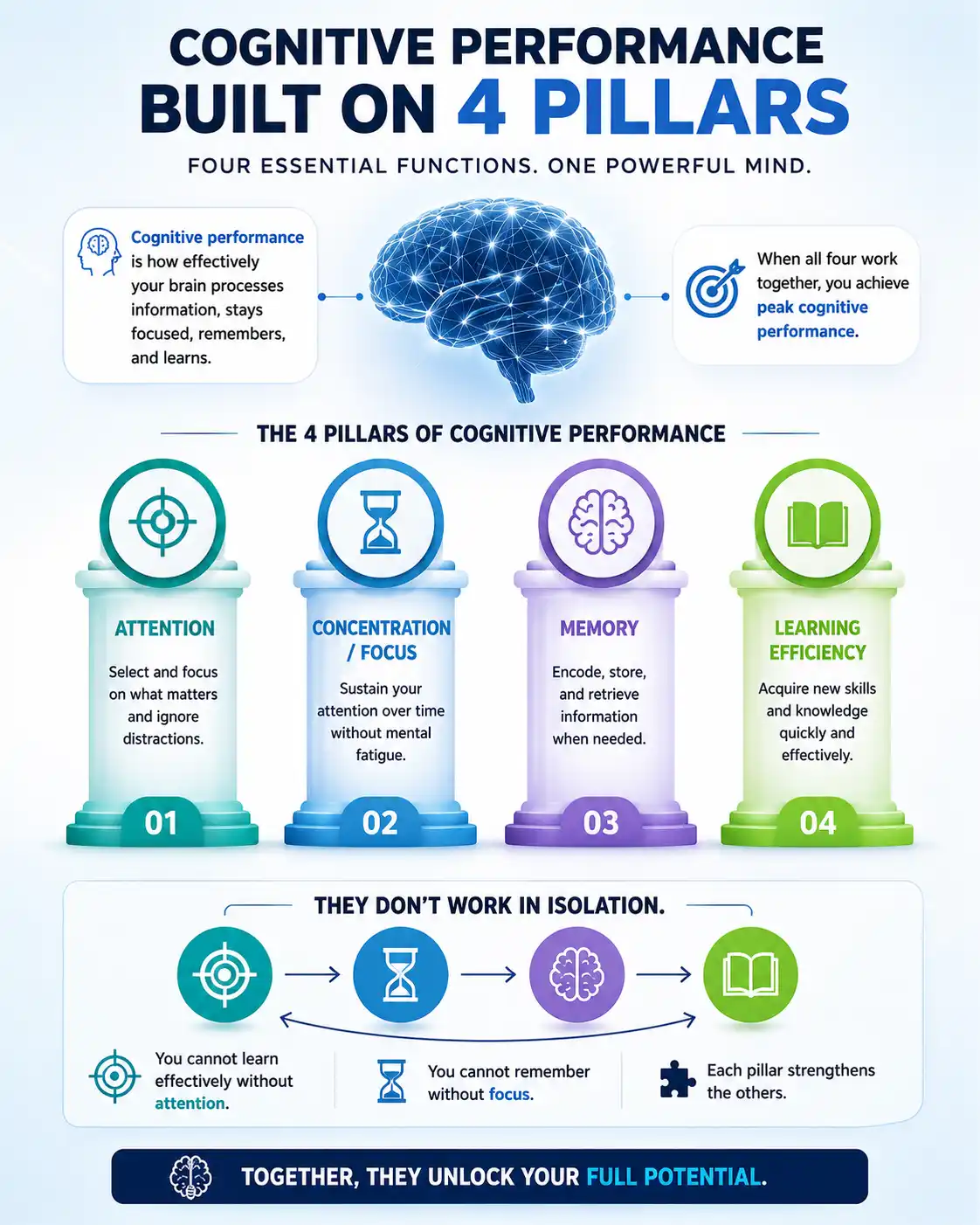
These four pillars do not work in isolation. They depend on each other. You cannot learn effectively without attention. You cannot remember without focus. When all four work together, you achieve peak cognitive performance.
Now, let us explore how neurofeedback can enhance each of these functions – and which BrainBit device is best for your needs.
How the Brain Supports Attention and Concentration
What the Brain Needs for Focus
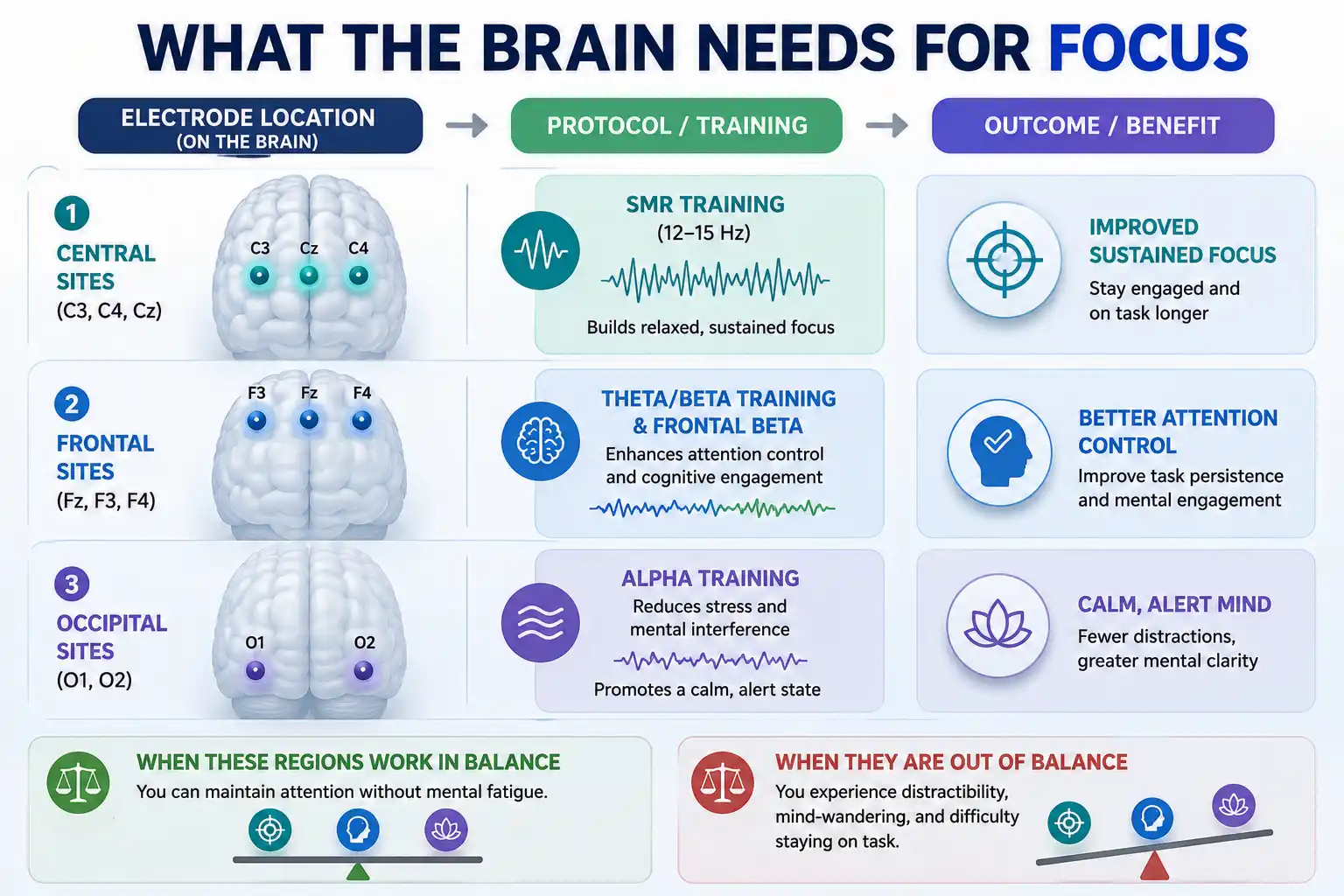
Attention and concentration rely on specific brain networks that work together to keep you engaged and alert. The key regions involved include:
- Central sites (C3, C4, Cz) – These are the primary locations for SMR training (12–15 Hz), the brainwave pattern associated with relaxed, sustained focus. SMR training is one of the most established protocols for attention enhancement.
- Frontal sites (Fz, F3, F4) – These regions support attention control, cognitive engagement, and task persistence. They are the target for Theta/Beta training and Frontal Beta enhancement.
- Occipital sites (O1/O2) – Alpha training at these sites reduces stress and mental interference that can impair concentration. It supports a calm, alert state that is conducive to sustained focus.
When these regions work in balance, you can maintain attention without mental fatigue. When they are out of balance, you experience distractibility, mind-wandering, and difficulty staying on task.
Protocol Recommendations for Attention and Concentration/Focus:
Based on clinical neurofeedback literature, the following protocols are effective for attention and concentration enhancement:
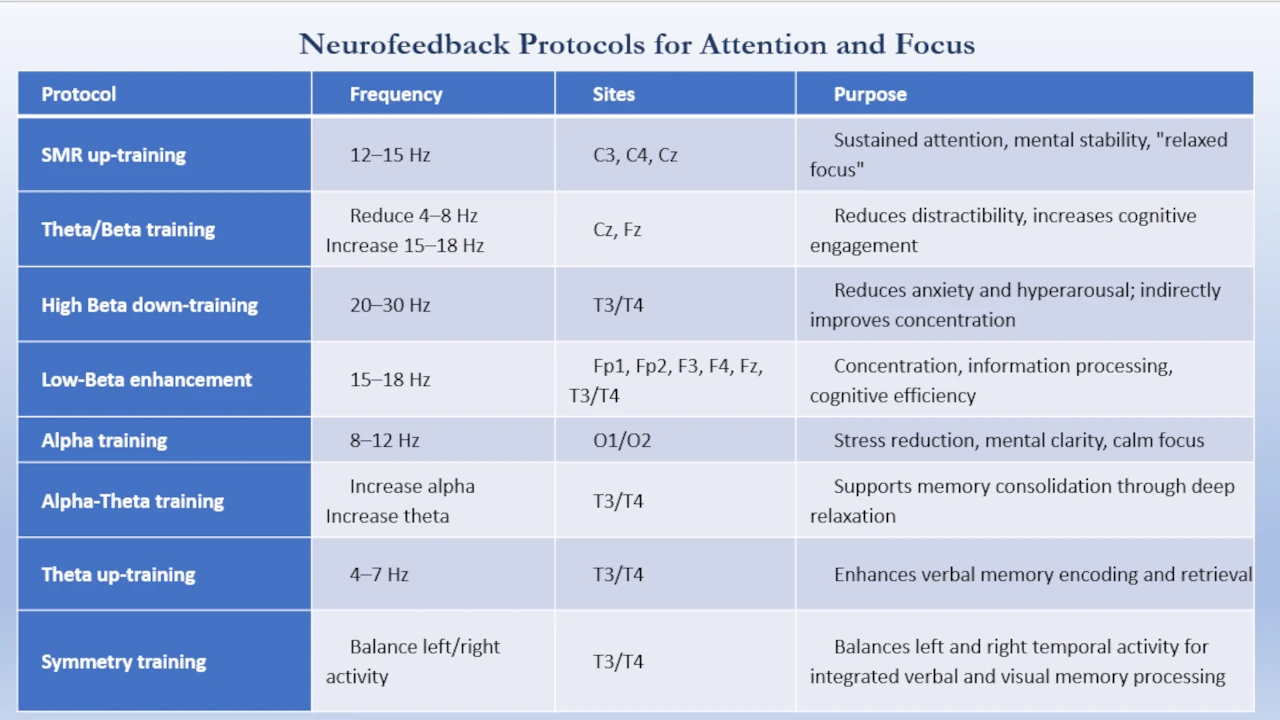
- SMR up-training (12–15 Hz) at C3, C4, or Cz – The most established protocol for sustained attention, mental stability, and “relaxed focus.” Frequently used for attention training and ADHD support.
- Theta/Beta training at Cz or Fz – Reduces excessive theta activity (associated with distractibility and mind-wandering) while increasing beta activity (associated with cognitive engagement). Commonly used for attention regulation.
- Frontal Low-Beta enhancement (15–18 Hz) at Fp1, Fp2, F3, F4, or Fz – Supports concentration, information processing, strengthens cognitive performance control, task persistence, and sustained attention during demanding cognitive work.
- Alpha training at O1/O2 – Reduces stress and mental interference that can impair concentration. Supports a calm, alert state conducive to sustained focus.
Which BrainBit Device Is Best for Attention and Concentration/Focus?
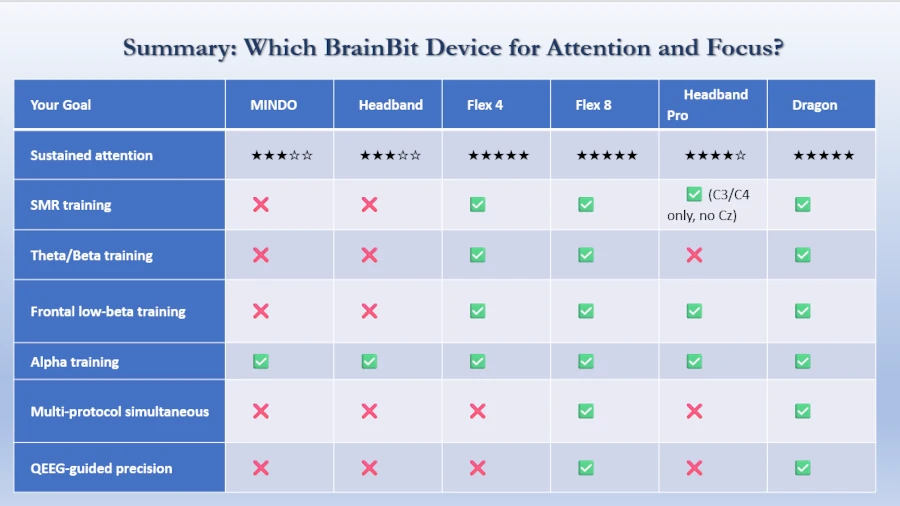
All BrainBit devices can support focus training, but they differ in how directly and effectively they target the underlying brain regions.
MINDO/Headband (★★★☆☆)
Available Protocols for MINDO/Headband:
- Beta enhancement at T3/T4 – Can train focus via beta enhancement at T3/T4. This is effective, but it is a unilateral approach. May cause anxiety in some users (see Clinical Note below)
- Alpha training at O1/O2 – Reduces stress and mental interference that can impair concentration. Supports a calm, alert state conducive to sustained focus
Limitations: No access to central SMR training sites (C3/C4/Cz). Cannot perform Theta/Beta training at Cz or Fz. No access to frontal sites (Fp1/Fp2, F3/F4, Fz).
Flex 4 (★★★★★)
With the 4-flexible-electrode placement system, Flex 4 electrodes can be placed at C3, C4, Cz, and Fz for comprehensive focus training.
Protocols:
- SMR up-training at C3, C4, or Cz – the most established protocol for sustained attention and “relaxed focus”
- Theta/Beta training at Cz or Fz – reduces distractibility and increases cognitive engagement
- Frontal Low-Beta enhancement at Fz – supports concentration and cognitive performance control
- Alpha training at O1/O2 can be added if you choose to place electrodes there (but this would replace other protocols)
Trade-off: You use all 4 electrodes for focus training, so you cannot simultaneously train other functions in the same session.
Flex 8 (★★★★★)
With the 8 flexible electrode placement system, Flex 8 electrodes can be placed for the following protocols:
- SMR up-training at C3, C4, and Cz
- Theta/Beta training at Cz and Fz
- Frontal Low-Beta enhancement at Fp1, Fp2, F3, and F4
- Alpha training at O1/O2 for stress reduction and mental clarity
Full central, frontal, and occipital coverage. Can train all attention and concentration protocols simultaneously. Allows combined focus + stress reduction for optimal concentration.
Headband Pro (★★★★☆)
Built-in C3/C4 (central) and Fp1/Fp2 (frontal). Headband Pro suitable for the following attention and concentration protocols:
- SMR up-training at C3 and C4
- Frontal Low-Beta enhancement at Fp1 and Fp2
- Alpha training at O1/O2 for stress reduction and mental clarity
Limitations: Missing Cz (the gold standard location for SMR training). Missing Fz, F3/F4. Cannot access Theta/Beta training at Cz or Fz.
Dragon EEG (★★★★★)
Full central, frontal, and occipital coverage with 21 channels. Dragon EEG can perform all protocols listed above simultaneously. QEEG mapping can identify specific central or frontal asymmetries that may affect attention and tailor protocols accordingly.
Decision Framework for Each BrainBit Device to Improve Attention and Focus
MINDO/Headband
Step 1: Identify Your Primary Challenge
- Difficulty with sustained focus?
- Difficulty with concentration under stress?
- Anxiety interfering with attention?
Step 2: Select Your Protocol
| If Your Primary Goal Is... | Protocol | Electrode Position | Why This Works |
|---|---|---|---|
Focus and concentration |
Beta enhancement at T3/T4 |
Fixed (T3, T4) |
Targets temporal beta activity associated with cognitive engagement |
Stress-related attention difficulties |
Alpha training at O1/O2 |
Fixed (O1, O2) |
Reduces stress and mental interference that impair concentration |
Clinical Note: Beta training at T3/T4 can be effective but may cause anxiety in some users. For users prone to anxiety, start with Alpha training at O1/O2 to establish a calm baseline before adding beta training.
Flex 4
Step 1: Identify Your Primary Challenge
- Difficulty with sustained focus and attention?
- Difficulty with distractibility or mind-wandering?
- Difficulty with concentration under stress?
Step 2: Select Your Protocol and Electrode Placement
| If Your Primary Goal Is... | Protocol | Electrode Montage | Why This Works |
|---|---|---|---|
Sustained attention and “relaxed focus” |
SMR up-training (12–15 Hz) |
C3, C4, Cz, Fz |
SMR training promotes mental stability and sustained attention without anxiety |
Distractibility and mind-wandering |
Theta/Beta training (4–8 Hz down / 15–18 Hz up) |
Cz, Fz, C3, C4 |
Reduces theta activity associated with mind-wandering while increasing beta for cognitive engagement |
Concentration under stress |
Alpha training (8–12 Hz) at O1/O2 + SMR at C3/C4 |
O1, O2, C3, C4 |
Combines stress reduction with sustained attention |
Trade-off: You choose one protocol per session.
Flex 8
Step 1: Identify Your Focus Challenges
Flex 8 allows multiple protocols simultaneously. Use this if you have multiple attention challenges.
Step 2: Select Your Protocol Combination
| If Your Primary Goal Is... | Protocol | Electrode Montage | Why This Works |
|---|---|---|---|
Focus + Stress Reduction |
SMR up-training + Alpha training |
C3, C4, Cz, + O1, O2 |
SMR for sustained attention, Alpha for stress reduction |
Focus + Cognitive Control |
SMR up-training + Frontal Low-Beta enhancement |
C3, C4, Cz, + Fp1, Fp2 |
SMR for attention, frontal beta for task persistence |
Full Attention Optimization |
SMR + Theta/Beta + Frontal Low-Beta + Alpha |
C3, C4, Cz,+ Fz, Fp1, Fp2, + O1, O2 |
Comprehensive coverage for all attention protocols |
Headband Pro
Step 1: Identify Your Primary Challenge
- Focus and sustained attention?
- Distractibility and task persistence?
Step 2: Select Your Protocol and Montage
| If Your Primary Goal Is... | Protocol | Electrode Montage | Why This Works |
|---|---|---|---|
Sustained attention |
SMR up-training at C3/C4 + Alpha training at O1/O2 |
Central strap (C3, C4) and O1, O2 |
SMR for sustained attention, Alpha for stress reduction |
Cognitive control and task persistence |
Frontal Low-Beta enhancement at Fp1/Fp2 + Alpha at O1/O2 |
Frontal + Occipital (Fp1, Fp2, O1, O2) |
Frontal beta for cognitive control, Alpha for mental clarity |
Limitations: Headband Pro cannot access Cz (the gold-standard location for SMR training) or Fz (the gold-standard location for Theta/Beta training). C3/C4 SMR remains effective but is less optimal than Cz.
Dragon EEG
Step 1: QEEG Assessment First (Recommended)
“Without QEEG assessment, you are guessing. With QEEG, you are training with precision.”
Before any training, perform a QEEG brain map to identify:
- Which brain regions are overactive or underactive during attention tasks
- Specific central or frontal asymmetries affecting focus
- Individual brainwave patterns affecting attention
Step 2: Use QEEG Data to Select Your Protocol
| If QEEG Shows... | This Means... | Your Protocol Should Be... |
|---|---|---|
Reduced SMR (12–15 Hz) at C3/C4/Cz |
Low sustained attention capacity |
SMR up-training at C3/C4/Cz |
Excessive theta (4–7 Hz) at Cz/Fz |
High distractibility and mind-wandering |
Theta/Beta training at Cz/Fz |
Reduced low-beta (15–18 Hz) at Fp1/Fp2 |
Low cognitive control and task persistence |
Frontal Low-Beta enhancement at Fp1/Fp2 |
Excessive high-beta (20–30 Hz) at frontal sites |
Anxiety interfering with attention |
High-Beta down-training at Fp1/Fp2 |
Reduced alpha (8–12 Hz) at O1/O2 |
Stress and mental interference impairing focus |
Alpha training at O1/O2 |
Step 3: Comprehensive Multi-Region Training
With 21 channels, Dragon EEG can train all attention protocols simultaneously:
- SMR up-training at C3/C4/Cz (sustained attention)
- Theta/Beta training at Cz/Fz (reduced distractibility)
- Frontal Low-Beta enhancement at Fp1/Fp2 (cognitive control)
- Alpha training at O1/O2 (stress reduction)
All in the same session.
Step 4: Track Progress
Use Dragon EEG’s QEEG capabilities to:
- Monitor changes in attention-related brain activity over time
- Adjust protocols based on objective data
- Generate reports showing attention improvements
How the Brain Supports Memory - Improve Cognitive Performance
What the Brain Needs for Memory
Memory is not a single function. It depends on multiple brain regions working together:
- Temporal sites (T3/T4) – Verbal memory (names, facts, spoken information)
- Temporal sites (T5/T6) – Visual memory (faces, places, spatial information)
- Occipital sites (O1/O2) – Alpha relaxation that reduces mental interference during encoding and recall
- Parietal sites (P3/P4) – Short-term memory and recall (T3-P3, T3-T5); mathematics and spatial memory (T4-P4)
When these regions work in balance, you can encode, store, and retrieve information efficiently. When they are out of balance, you experience memory lapses, forgetting, and difficulty learning new material.
Neurofeedback Protocols for Memory Enhancement
Based on clinical neurofeedback literature, the following protocols are effective for memory enhancement:
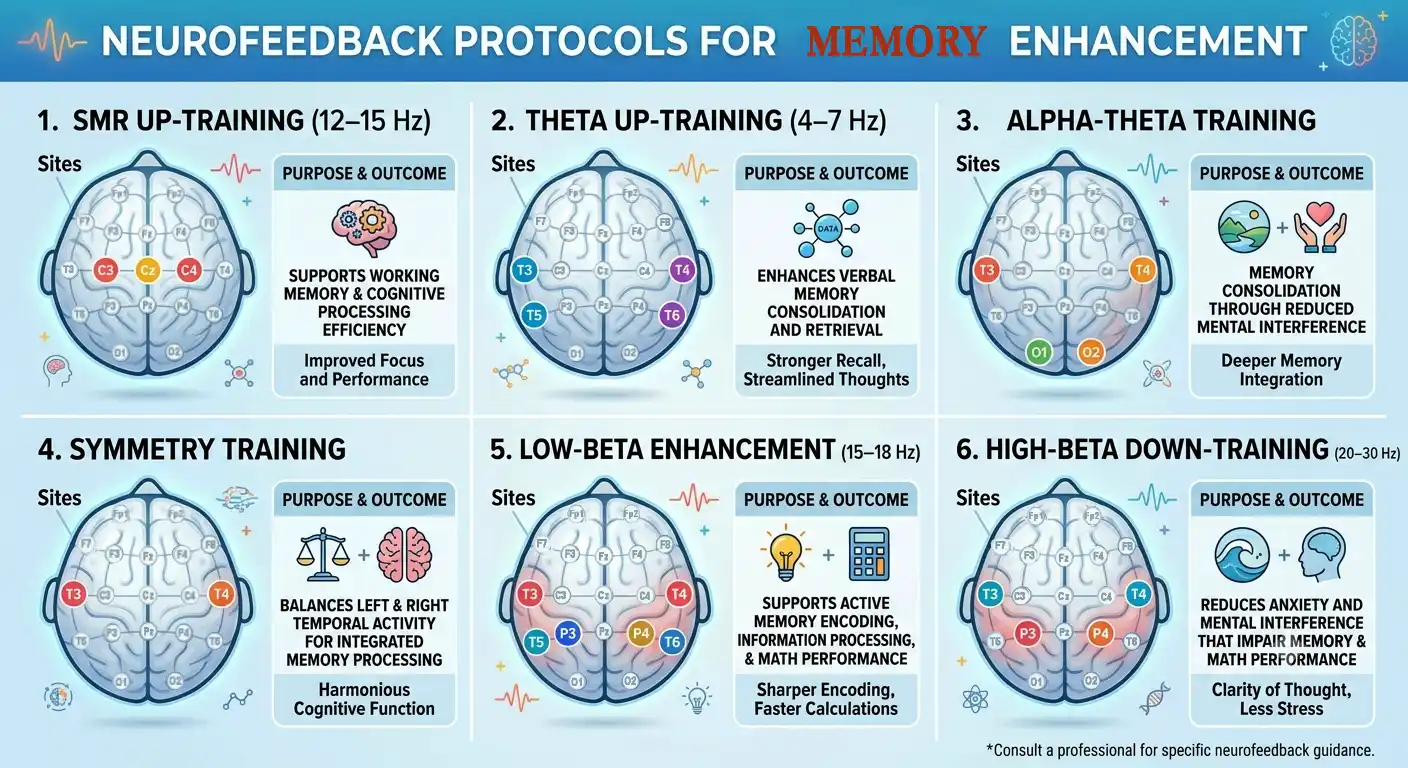
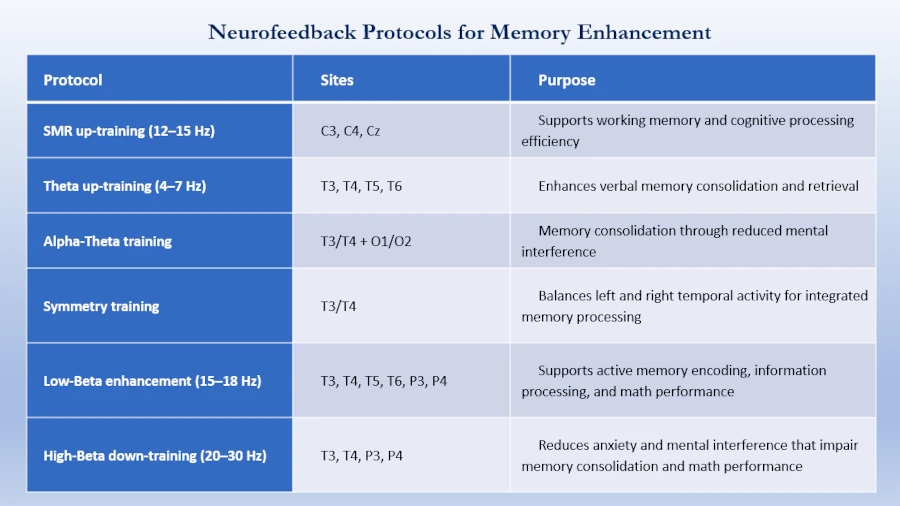
- Low-beta enhancement at T3-T5 and T3-P3 – targets the temporal‑parietal network, which stores and retrieves verbal memories. Consequently, this protocol improves short‑term memory and recall.
- High-Beta down training at T4-P4 – targets the right temporal‑parietal network, which supports spatial memory and numerical processing. As a result, this training boosts memory and mathematical performance.
- Theta up-training (4–7 Hz) at temporal sites – Research demonstrates that increasing theta power during memory encoding enhances verbal memory consolidation and retrieval. Studies using intracranial EEG have shown that theta activity in the medial temporal lobe during encoding promotes subsequent memory function.
- Alpha-theta training at T3/T4 with O1/O2 – Combining temporal training with occipital Alpha supports memory consolidation through reduced mental interference during encoding.
- Symmetry training between T3 and T4 – Training for balanced activity between left and right temporal lobes supports integrated verbal and visual memory processing. Asymmetry in temporal activity can indicate inefficient memory encoding.
- SMR up-training (12–15 Hz) at C3/C4 or Cz – While primarily associated with sustained attention and focus, SMR training also supports working memory and cognitive processing efficiency. This protocol is most effective when used at central sites.
Which BrainBit Device Is Best for Memory Training and Cognitive Performance Improvement?
MINDO / Headband (★★★★☆):
Because both of them have 4 fixed electrodes at T3, T4 and O1, O2, they can improve memory through the following training:
- Theta up-training (4–7 Hz) at T3/T4 for verbal memory
- Alpha-Theta training at T3/T4 for verbal memory + Alpha relaxation training at O1/O2 for memory consolidation
- Symmetry training at T3/T4, combined with alpha training at O1 and O2, promotes balanced activity between the left and right temporal lobes. Consequently, this integration supports both verbal and visual memory processing. However, temporal asymmetry often signals inefficient memory encoding.
- Low-Beta enhancement (15–18 Hz) at T3/T4 – active memory encoding
- High-Beta down-training (20–30 Hz) at T3/T4 – reduces anxiety that impairs memory
- Although these devices cannot be used for T3-T5, T3-P3, or T4-P4 protocols, they are still very effective for verbal memory and memory-related relaxation.
Limitations: Cannot access T5/T6 for visual memory. Cannot access parietal sites (P3/P4) for T3-P3 or T4-P4 derivations.
Flex 4 (★★★★★):
Because of the 4 flexible electrode placement system, they can be placed for the following protocols to improve memory:
- Symmetry training between T3 and T4 + Alpha training at O1/O2 – Balances left and right temporal activity while supporting memory consolidation through relaxation
- T3/T4 Alpha-Theta training or Theta up-training + Alpha training at O1/O2 – Enhances verbal memory consolidation and encoding with reduced mental interference
- T3, T4, T5, and T6 – full temporal coverage. You can then choose from several protocols. For instance, Alpha-Theta training supports memory consolidation. Meanwhile, Theta up-training enhances encoding, and Alpha up-training reduces interference. Alternatively, Low-Beta enhancement strengthens active memory encoding.
- T3-T5, T4-P4, and T3-P3 protocols offer comprehensive training for memory and mathematics. Specifically, you may use Theta up-training, Alpha-Theta training, or SMR training to boost cognitive processing efficiency. Moreover, Low-Beta enhancement improves active memory encoding and math performance. In contrast, High-Beta down-training reduces anxiety and mental interference, both of which impair memory consolidation.
Can place electrodes at T3/T4, T5/T6, or P3/P4 for comprehensive memory training.
Trade-off: You use all 4 electrodes for memory training, so you cannot simultaneously train other functions in the same session.
Decision Framework for Flex 4 Memory Training to Boost Cognitive Performance
For a Flex 4 user, the decision is a two-step process. Because you have four flexible electrodes, you can only perform one protocol at a time. This framework guides you from your primary goal to the optimal protocol and placement.
Step 1: Identify Your Primary Goal
You should first identify your core memory-related challenge.
- Difficulty remembering verbal information? (e.g., names, facts, spoken instructions)
- Difficulty with visual-spatial information? (e.g., faces, directions, numerical data)
- Difficulty remembering information under stress or anxiety?
- Difficulty with processing speed and concentration while learning?
Step 2: Select Your Protocol and Electrode Placement
Based on your answer, you can select the specific protocol and placement using the table below.
| If Your Primary Goal Is... | Choose This Protocol | Place Electrodes At... | Why This Works |
|---|---|---|---|
Verbal Memory Enhancement
(Names, facts, spoken info) |
Theta Up-Training (4–7 Hz) |
T3 and T4
(Left and Right Temporal Lobes) |
This protocol enhances verbal memory consolidation and retrieval, making it easier to encode and recall spoken or read information. |
Visual Memory & Math Performance
(Faces, places, numbers) |
Low-Beta Enhancement (15–18 Hz) |
T5 and T6
(Left and Right Posterior Temporal Lobes) |
T5/T6 are associated with visual processing and numerical ability. Low-Beta training supports active encoding and processing of visual-spatial information. |
Memory with Anxiety/Overthinking
(Stress impairs recall) |
High-Beta Down-Training (20–30 Hz) |
T3 and T4
(Left and Right Temporal Lobes) |
High-Beta is associated with anxiety. Down-training it reduces mental interference and helps calm the nervous system, creating a better environment for memory consolidation. |
General Cognitive Efficiency
(Processing speed, focus) |
SMR Up-Training (12–15 Hz) |
C3 and C4
(Left and Right Central Cortex) |
Sensorimotor Rhythm (SMR) training is linked to a state of “relaxed focus.” It supports working memory and overall cognitive processing efficiency. |
General Recommendations for Flex 4 Users
As your training progresses, your needs may shift. Here are additional considerations:
- Start with the Most Specific Goal: Choose the protocol that directly targets your most significant challenge. For example, if you are a student who needs to memorize facts, start with Theta Up-Training at T3/T4.
- Address Anxiety First: If you consistently find that anxiety or overthinking primarily obstructs recall, start with High-Beta Down-Training at T3/T4 instead. Thereafter, once you establish a calmer baseline, you will likely improve memory consolidation.
- Progress to Combined Training: Once you make progress on one primary goal, switch to Combined Training in future sessions. This way, you can train other aspects of cognitive performance as well.
Consequently, this structured approach lets you navigate the Flex 4 system’s flexibility. Ultimately, you can make an informed decision based on your personal needs.
Flex 8 (★★★★★):
Because of the 8 flexible electrode placement system, they can be placed for the following protocols to improve memory:
- Symmetry training between T3 and T4
- T3/T4 Alpha-theta training or Theta up-training
- T3, T4, T5, and T6 – To achieve full temporal coverage, use protocols that target memory processing. For example, Alpha-Theta training supports memory consolidation. Likewise, Theta up-training enhances encoding, and Alpha up-training reduces interference.
- T3-T5, T4-P4, and T3-P3 protocols offer comprehensive memory training. Specifically, you can choose Theta up-training, Alpha-Theta training, or SMR training to boost cognitive efficiency.
- Alpha training can be performed simultaneously at O1/O2, which will reduce mental interference during encoding and recall.
- Highly effective. Allows simultaneous memory + relaxation protocols for optimal memory consolidation.
Decision Framework for Flex 8 Memory Training
The Flex 8 has 8 flexible electrodes. This means you can train multiple brain regions and protocols simultaneously, which is ideal for complex, multi-network memory training.
This framework guides you from your primary goal to the optimal combination of protocols and placements.
Step 1: Identify Your Primary Goal
The user should first identify their core memory-related challenge.
- Difficulty remembering verbal information? (e.g., names, facts, spoken instructions)
- Difficulty with visual-spatial information? (e.g., faces, directions, numerical data)
- Difficulty remembering information under stress or anxiety?
- Difficulty with processing speed and concentration while learning?
Step 2: Select Your Protocol Combination and Electrode Placement
For the Flex 8, you can combine protocols because you have enough electrodes to cover multiple regions. The table below suggests optimal combinations based on the primary goal.
| If Your Primary Goal Is... | Combine These Protocols | Place Electrodes At... | Why This Combination Works |
|---|---|---|---|
Verbal Memory Enhancement
(Names, facts, spoken info) | 1. Theta Up-Training (4–7 Hz) | 1.T3 and T4 for Theta up-training |
Theta up-training enhances verbal memory consolidation and retrieval, while Alpha training reduces mental interference during encoding. |
Visual Memory & Math Performance
(Faces, places, numbers) | 1. Low-Beta Enhancement (15–18 Hz) | 1.T5 and T6 for Low-Beta enhancement |
T5/T6 are associated with visual processing and numerical ability. Low-Beta training supports active encoding, while SMR training at C3/C4 supports working memory and cognitive processing efficiency. |
Memory with Anxiety/Overthinking
(Stress impairs recall) | 1. High-Beta Down-Training (20–30 Hz) | 1.T3 and T4 for High-Beta down-training |
High-Beta down-training reduces anxiety and mental interference. Theta up-training then enhances memory consolidation in a calmer state. |
General Cognitive Efficiency
(Processing speed, focus) | 1. SMR Up-Training (12–15 Hz) | 1.C3 and C4 for SMR training |
Sensorimotor Rhythm (SMR) training is linked to a state of “relaxed focus.” It supports working memory and overall cognitive processing efficiency. |
General Recommendations for Flex 8 Users
The Flex 8’s ability to run multiple protocols simultaneously provides more flexibility for advanced training.
- Start with the Most Specific Goal: Choose the protocol combination that most directly targets your most significant challenge.
- Address Anxiety First: If you find that anxiety or overthinking is the primary obstacle to recall, it is often more effective to start with High-Beta Down-Training at T3/T4 in combination with Alpha training.
- Progress to Combined Training: Once you have established a baseline on one primary goal, you can switch protocol combinations in future sessions to train other aspects of cognitive performance.
This structured approach allows you to leverage the full capabilities of the Flex 8 system and make an informed decision based on your personal needs.
Headband Pro (★★★★★):
Built-in T3, T4, T5, and T6. Full temporal coverage out of the box. It also has built-in O1 and O2 electrodes. So it is suitable for the following memory improvement protocols:
- Symmetry training between T3 and T4
- T3/T4 Alpha-theta training or Theta up-training
- T3, T4, T5, and T6 – achieving full temporal coverage. Protocols: Alpha-theta training, Theta up-training, or Alpha up-training
- Alpha training can be performed simultaneously at O1/O2, which will reduce mental interference during encoding and recall.
Although it cannot be used for the T4-P4 and T3-P3 protocols (which lack parietal electrodes), it remains highly effective for verbal memory and memory-related relaxation.
Decision Framework for Headband Pro Memory Training
The Headband Pro is an 8-channel EEG headband with fixed electrode positions. Unlike Flex 4 or Flex 8, you cannot move electrodes to different locations. Instead, you choose which available protocol to train using the existing electrode montage.
Available Electrode Montages
| Montage | Electrode Positions | When to Use |
|---|---|---|
Default (Temporal + Occipital) |
T3, T4, T5, T6, O1, O2 |
Standard memory, language, and relaxation training |
Central Strap Option |
C3, C4, T5, T6, O1, O2 |
SMR training for working memory and cognitive processing efficiency |
Frontal + Temporal + Occipital |
Fp1, Fp2, T3, T4, O1, O2 |
Emotional regulation, verbal memory, and relaxation |
Step 1: Identify Your Primary Goal
- Difficulty remembering verbal information? (names, facts, spoken instructions)
- Difficulty with visual-spatial information? (faces, directions, numerical data)
- Difficulty with working memory, processing speed, or concentration?
- Difficulty remembering information under stress or anxiety?
Step 2: Select Your Protocol and Electrode Montage
| If Your Primary Goal Is... | Combine These Protocols | Electrode Montage | Why This Combination Works |
|---|---|---|---|
Verbal Memory Enhancement
(Names, facts, spoken info) |
Theta Up-Training (4–7 Hz) at T3/T4 |
Default Montage
T3, T4, O1, O2 |
Theta up-training at T3/T4 enhances verbal memory consolidation and retrieval. Alpha training at O1/O2 reduces mental interference during encoding. |
Visual Memory & Math Performance
(Faces, places, numbers) |
Low-Beta Enhancement (15–18 Hz) at T5/T6 |
Default Montage
T5, T6, O1, O2 |
T5/T6 are associated with visual processing and numerical ability. Low-Beta training supports active encoding and processing of visual-spatial information. |
Working Memory & Cognitive Efficiency
(Processing speed, focus) |
SMR Up-Training (12–15 Hz) at C3/C4 |
Central Strap Montage
C3, C4, T5, T6, O1, O2 |
Sensorimotor Rhythm (SMR) training supports working memory and cognitive processing efficiency. Central sites (C3/C4) are associated with sustained attention and “relaxed focus.” |
Memory with Anxiety/Overthinking
(Stress impairs recall) |
High-Beta Down-Training (20–30 Hz) at T3/T4 + Alpha Training at O1/O2 |
Default Montage
T3, T4, O1, O2 |
High-Beta down-training reduces anxiety and mental interference. Alpha training provides relaxation and mental clarity, supporting memory consolidation. |
Emotional Memory Regulation
(Anxiety, rumination, mood) |
Frontal Alpha Asymmetry Training (Fp1/Fp2) + Alpha-Theta Training (T3/T4 + O1/O2) |
Frontal + Temporal + Occipital
Fp1, Fp2, T3, T4, O1, O2 |
Frontal Alpha Asymmetry training balances left and right frontal activity, supporting emotional regulation. Alpha-Theta training at temporal sites supports memory consolidation through deep relaxation. |
General Recommendations for Headband Pro Users
The Headband Pro’s fixed electrode positions mean you cannot change electrode locations, but you can change which montage and protocol you use for training.
- Start with the Default Montage: The standard montage (T3, T4, T5, T6, O1, O2) covers the primary memory-related regions. Begin here for most memory training goals.
- Switch to Central Strap for Working Memory: If your primary challenge is processing speed, concentration, or working memory, use the central strap option to record from C3/C4 for SMR training.
- Add Frontal Sites for Emotional Regulation: If anxiety or overthinking is the primary obstacle to recall, use the frontal + temporal + occipital montage (Fp1, Fp2, T3, T4, O1, O2) to combine emotional regulation with memory training.
Dragon (★★★★★):
The Dragon EEG is a 21-channel professional EEG system with full 10–20 head coverage. Unlike other BrainBit devices, Dragon EEG is designed for quantitative EEG (qEEG) assessment and research. Its primary advantage is not just training, but understanding your brain first through comprehensive brain mapping.
Available Electrode Coverage
- Frontal – Fp1, Fpz, Fp2, F7, F3, Fz, F4, F8
- Central – C3, Cz, C4
- Temporal – T3, T4, T5, T6
- Parietal – P3, Pz, P4
- Occipital – O1, Oz, O2
- Additional Channels: 3 poly channels for EMG, ECG, and EOG measurements
Decision Framework for Dragon EEG Memory Training
Step 1: Identify Your Primary Goal
- Difficulty remembering verbal information? (names, facts, spoken instructions)
- Difficulty with visual-spatial information? (faces, directions, numerical data)
- Difficulty with working memory, processing speed, or concentration?
- Difficulty remembering information under stress or anxiety?
- Want to understand your brain’s unique memory patterns before training?
Step 2: Choose Your Approach
The Dragon EEG offers two distinct approaches:
Approach A: QEEG Assessment First (Recommended)
“Without QEEG assessment, you are guessing. With QEEG, you are training with precision.”
Before any training, perform a QEEG brain map to identify:
- Which brain regions are overactive or underactive
- Specific temporal or parietal asymmetries
- Individual brainwave patterns affecting memory
This gives you a personalized “brain blueprint” to guide all subsequent training.
How to Use QEEG Data to Select Your Protocol for Memory Training and Cognitive Performance Improvement
Once you have your QEEG report, use the following logic to determine which protocol to train:
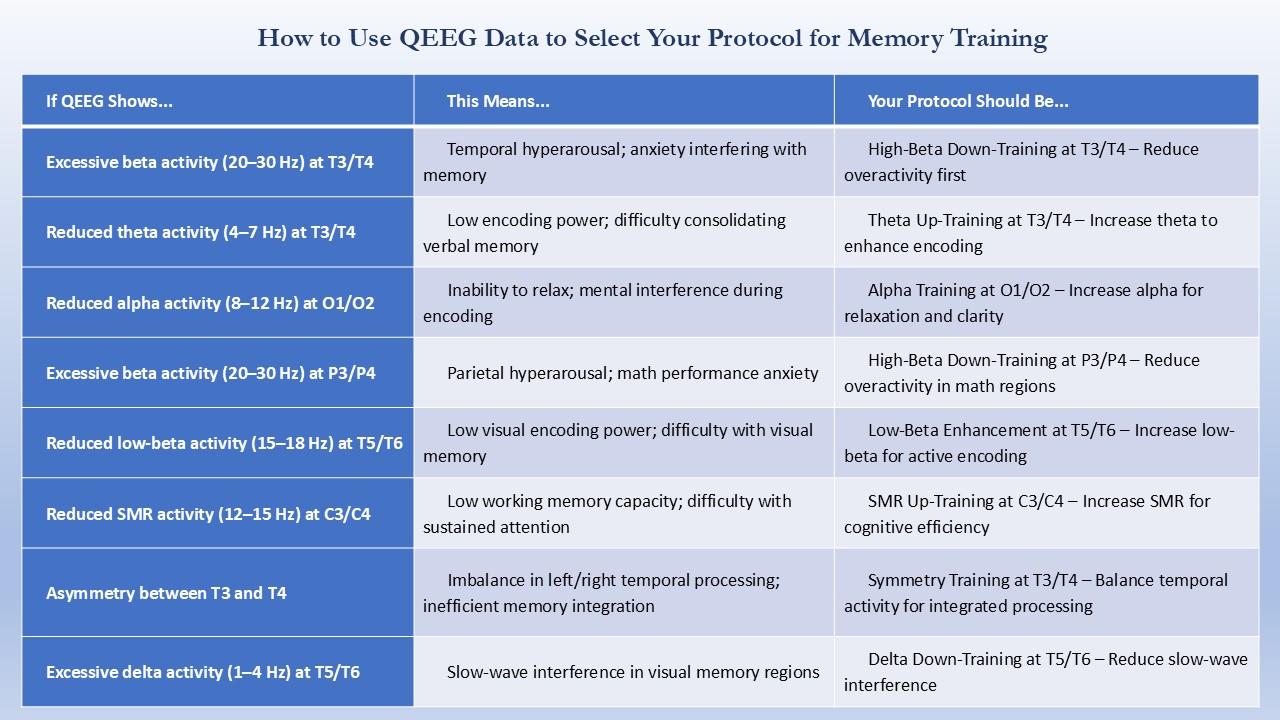
Practical Example
QEEG Finding:
Increased beta activity (20–30 Hz) at T3/T4 + reduced theta activity (4–7 Hz) at T3/T4
Interpretation:
Temporal hyperarousal is interfering with verbal memory encoding.
Action:
- First – High-Beta Down-Training at T3/T4 (reduce anxiety/overactivity)
- Then – Theta Up-Training at T3/T4 (enhance verbal memory encoding)
Why This Matters
Without QEEG
- Guessing which protocol to use
- Potentially training the wrong region
- Wasting time on ineffective protocols
- Risk of side effects (e.g., anxiety from beta training)
With QEEG
- Training based on your actual brain activity
- Targeting exactly what needs improvement
- Maximizing training efficiency
- Avoiding protocols that may worsen your specific pattern
Who Benefits Most from QEEG-Guided Training?
| User Type | Benefit |
|---|---|
Complex memory issues |
Identifies root causes, not just symptoms |
Treatment-resistant cases |
Finds patterns missed by generic protocols |
Researchers |
Provides objective baseline and outcome data |
Advanced home users |
Precision training with professional-grade insights |
Approach B: Direct Neurofeedback Training
After assessment, use the full 21-channel system to run comprehensive memory protocols.
Step 3: Select Your Protocol Combination
With 21 electrodes, you can train multiple memory-related regions simultaneously.
| If Your Primary Goal Is... | Combine These Protocols | Place Electrodes At... | Why This Combination Works |
|---|---|---|---|
Verbal Memory Enhancement
(Names, facts, spoken info) | 1. Theta Up-Training (4–7 Hz) | 1.T3, T4 for Theta up-training |
Theta up-training enhances verbal memory consolidation. Alpha training reduces mental interference. Symmetry training balances temporal activity for integrated processing. |
Visual Memory & Math Performance
(Faces, places, numbers) | 1. Low-Beta Enhancement (15–18 Hz) | 1.T5, T6 for Low-Beta |
T5/T6 support visual processing and numerical ability. SMR at C3/C4 supports working memory. P3/P4 down-training reduces anxiety that impairs math performance. |
Memory with Anxiety/Overthinking
(Stress impairs recall) | 1. High-Beta Down-Training (20–30 Hz) | 1.T3, T4 for High-Beta down-training |
High-Beta down-training reduces anxiety and mental interference. Theta up-training then enhances memory consolidation in a calmer state. Alpha training provides relaxation. |
General Cognitive Efficiency
(Processing speed, focus) | 1. SMR Up-Training (12–15 Hz) | 1.C3, C4 for SMR
|
SMR supports working memory. Alpha provides stress reduction and mental clarity. Frontal Low-Beta enhances cognitive control and task persistence. |
Step 4: Advanced Options
Option 1: T3-P3 and T4-P4 Protocols
Dragon EEG’s full parietal coverage enables T3-P3 (short-term memory and recall) and T4-P4 (memory and mathematics) protocols. These are not available on Headband Pro (missing P3/P4) and require multiple electrodes on Flex devices.
Option 2: QEEG-Guided Protocol Selection
Use Dragon EEG’s qEEG capabilities to:
- Compare your brain activity against normative databases
- Identify specific asymmetries affecting memory
- Tailor protocols to your unique brain patterns
- Track changes over time with quantitative reports
Option 3: Simultaneous Multi-Region Training
With 21 channels, you can train:
- Verbal memory (T3/T4)
- Visual memory (T5/T6)
- Working memory (C3/C4)
- Emotional regulation (Fp1/Fp2)
- Relaxation (O1/O2)
All in the same session.
Key Advantage of Dragon EEG
The Dragon EEG is the only BrainBit device that combines:
- Full 10-20 coverage – 21 channels across the entire head
- QEEG assessment – Compare your brain against normative databases
- EMG/ECG/EOG channels – Artifact control and synchronized HRV biofeedback
- EDF/CSV export – Professional analysis in NeuroGuide and BrainAssistant
- All protocols simultaneously – Train memory, attention, and emotional regulation in one session
This makes Dragon EEG the most comprehensive single-device solution for memory training and cognitive assessment.
How the Brain Supports Learning Efficiency
What the Brain Needs for Learning
Learning efficiency is the ability to acquire new skills and knowledge quickly and effectively. In particular, it depends on attention, memory, and cognitive flexibility working together. Moreover, several key brain regions support this process.
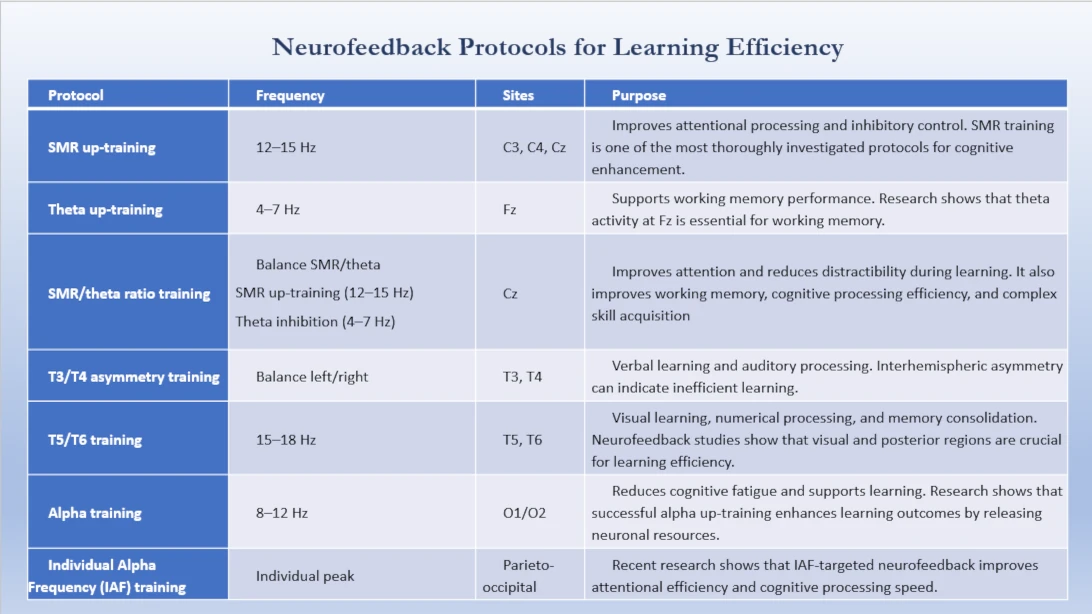
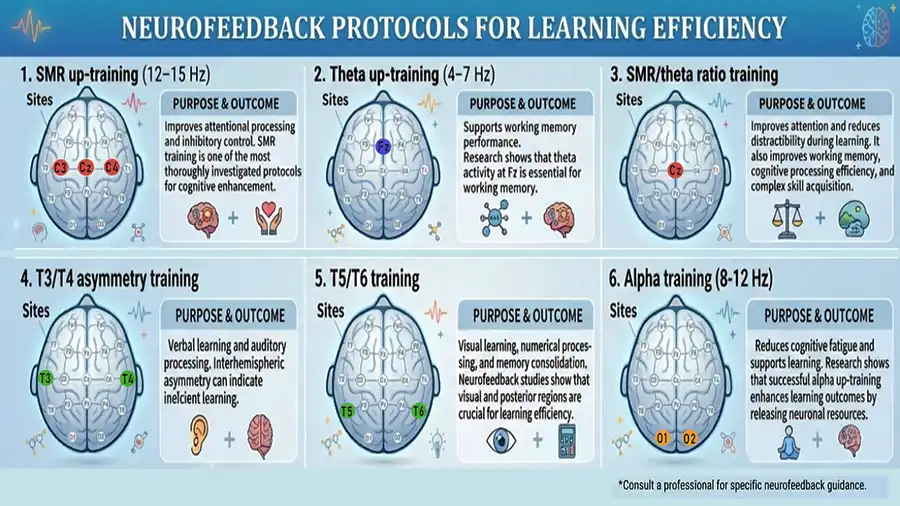
- Central sites (C3, C4, Cz) – SMR up-training (12–15 Hz) supports sustained attention and cognitive processing. SMR training is the most established protocol for attentional processing and inhibitory control, which are essential for learning.
- Frontal sites (Fp1, Fp2, Fz) – Executive function and working memory. Theta activity (4–7 Hz) at Fz is associated with working memory performance, which is critical for learning.
- Temporal sites (T3/T4) – Verbal learning and auditory processing. Studies show that the temporal lobes play a crucial role in memory encoding and retention.
- Posterior temporal sites (T5/T6) – Visual learning, numerical processing, and information integration.
- Occipital sites (O1/O2) – Alpha training reduces cognitive fatigue and supports relaxation during learning tasks. Research demonstrates that alpha oscillations regulate information flow in the brain and that successful alpha up-training enhances learning outcomes.
- SMR/theta ratio training (Cz) – Balance SMR/theta – Improves attention and reduces distractibility during learning.
The SMR/theta ratio protocol works through two complementary mechanisms:
- SMR up-training (12–15 Hz) enhances sustained attention, perceptual sensitivity, and cognitive performance. In fact, research shows that SMR training improves attentional processing, working memory, and inhibitory control.
- Theta inhibition (4–7 Hz) – In contrast, theta inhibition (4–7 Hz) reduces theta activity, which is associated with distractibility, mind-wandering, and inattention.
When these regions work together, you can absorb, process, and retain new information efficiently. When they are out of balance, learning becomes slow, difficult, and frustrating.
Neurofeedback Protocols for Learning Efficiency
Based on clinical neurofeedback literature, the following protocols are effective for learning efficiency:
Which BrainBit Device Is Best for Learning Efficiency?
MINDO / Headband (★★★☆☆)
Available Protocols:
- Alpha training at O1/O2 – reduces cognitive fatigue and supports learning
- T3/T4 asymmetry training – verbal learning and auditory processing
- T3/T4 SMR up-training – improves auditory perception
Limitations: However, you cannot access central sites (C3/C4/Cz) for SMR training. Likewise, frontal sites (Fz) are unavailable for theta up-training. Similarly, posterior temporal sites (T5/T6) remain inaccessible for visual learning.
Flex 4 (★★★★★)
Can place electrodes at C3/C4/Cz, Fz, T3/T4, T5/T6, or O1/O2.
Protocols:
- SMR up-training at C3, C4, or Cz – improves attentional processing and inhibitory control
- Theta up-training at Fz – supports working memory performance
- SMR/theta ratio training at Cz – improves attention and reduces distractibility
- T3/T4 asymmetry training – verbal learning and auditory processing
- T5/T6 training – visual learning, numerical processing, and memory consolidation
- Alpha training at O1/O2 – reduces cognitive fatigue
Trade-off: You use all 4 electrodes for learning support training, so you cannot simultaneously train other functions in the same session. With 4 electrodes, you must choose which protocol to run (e.g., SMR training, visual memory training, or verbal learning training) in each session.
Flex 8 (★★★★★)
Full central, frontal, temporal, posterior temporal, and occipital coverage. Can train all learning protocols simultaneously.
- SMR up-training at C3, C4, or Cz – improves attentional processing and inhibitory control
- Theta up-training at Fz – supports working memory performance
- SMR/theta ratio training at Cz – improves attention and reduces distractibility
- T3/T4 asymmetry training – verbal learning and auditory processing
- T5/T6 training – visual learning, numerical processing, and memory consolidation
- Alpha training at O1/O2 – reduces cognitive fatigue
Allows combined attention + working memory + verbal learning + visual learning + relaxation for comprehensive learning support.
Headband Pro (★★★★☆)
Built-in T3/T4, T5/T6, and O1/O2.
Protocols: T3/T4 asymmetry training, T5/T6 training, Alpha training at O1/O2.
Limitations: Unfortunately, the setup lacks C3/C4/Cz for SMR training. Likewise, Fz is missing for theta up-training. As a result, you cannot access central or frontal sites for attention and working memory training.
Dragon EEG (★★★★★)
Full central, frontal, temporal, posterior temporal, and occipital coverage with 21 channels. Can perform all protocols listed above simultaneously. QEEG mapping can identify specific central, frontal, or temporal asymmetries that may affect learning and tailor protocols accordingly.
Decision Framework for Each BrainBit Device to Boost Learning Efficiency
MINDO / Headband
Step 1: Identify Your Primary Learning Challenge
- Difficulty with verbal learning (reading, listening, spoken information)?
- Difficulty with sustained attention during learning?
- Difficulty relaxing or reducing cognitive fatigue during study?
Step 2: Select Your Protocol
| If Your Primary Goal Is... | Protocol | Electrode Montage | Why This Works |
|---|---|---|---|
Verbal learning | T3/T4 asymmetry training | Fixed (T3, T4, O1, O2) |
Balances left and right temporal activity for verbal learning and auditory processing |
Sustained attention during learning | T3/T4 SMR up-training | Fixed (T3, T4, O1, O2) |
SMR training at T3/T4 improves auditory perception and attentional processing |
Cognitive fatigue | Alpha training at O1/O2 | Fixed (O1, O2) |
Reduces cognitive fatigue and supports learning |
Flex 4
Step 1: Identify Your Primary Learning Challenge
- Difficulty with attention and focus during learning?
- Difficulty with working memory (holding information while processing)?
- Difficulty with verbal learning or auditory processing?
- Difficulty with visual learning or numerical processing?
Step 2: Select Your Protocol and Electrode Placement
| If Your Primary Goal Is... | Protocol | Place Electrode At... | Why This Works |
|---|---|---|---|
Verbal learning | T3/T4 asymmetry training | T3, T4 |
Balances left and right temporal activity for verbal learning and auditory processing |
Attention and focus during learning |
SMR up-training (12–15 Hz) |
C3, C4, Cz, Fz |
SMR training improves attentional processing and inhibitory control |
Working memory |
Theta up-training (4–7 Hz) |
Fz, Cz, C3, C4 |
Theta activity at Fz is essential for working memory performance |
Visual learning |
T5/T6 training (15–18 Hz) |
T5, T6, O1, O2 |
Posterior temporal sites are crucial for visual learning and numerical processing |
Trade-off: You choose one protocol per session.
Flex 8
Step 1: Identify Your Learning Challenges
Flex 8 allows multiple protocols simultaneously. Use this if you have multiple learning challenges.
Step 2: Select Your Protocol Combination
Trade-off: You choose one protocol per session.
| If Your Primary Goal Is... | Combine These Protocols | Place Electrode At... | Why This Works |
|---|---|---|---|
Attention + Verbal Learning + Relaxation | SMR up-training + T3/T4 asymmetry + Alpha training | C3, C4, T3, T4, O1, O2 |
SMR for sustained attention, T3/T4 asymmetry for verbal learning and auditory processing, Alpha training at O1/O2 for reduced cognitive fatigue |
Working Memory + Visual Learning |
Theta up-training + Low-Beta enhancement + Alpha training |
Fz, Cz, T5, T6, O1, O2 |
Theta up-training at Fz/Cz for working memory, Low-Beta enhancement at T5/T6 for visual encoding, Alpha training at O1/O2 for reduced cognitive fatigue |
All Learning Functions |
SMR up-training + Theta up-training + T3/T4 asymmetry + Low-Beta enhancement + Alpha training |
C3, C4, Fz, T3, T4, T5, T6, O1, O2 |
Comprehensive coverage combining attention (SMR), working memory (Theta), verbal learning (T3/T4), visual learning (Low-Beta at T5/T6), and cognitive fatigue reduction (Alpha at O1/O2) |
Headband Pro
Step 1: Identify Your Primary Learning Challenge
- Verbal learning (T3/T4)?
- Visual learning (T5/T6)?
- Cognitive fatigue (O1/O2)?
Step 2: Select Your Protocol and Montage
| If Your Primary Goal Is... | Protocol | Electrode Montage | Why This Works |
|---|---|---|---|
Verbal learning | T3/T4 asymmetry training | Default (T3, T4, O1, O2) |
Balances left and right temporal activity for verbal learning and auditory processing |
Visual learning | Low-Beta enhancement training – T5/T6 training (15–18 Hz) | Default (T5, T6, O1, O2) |
Posterior temporal sites for visual learning |
Cognitive fatigue | Alpha training at O1/O2 | Default (O1, O2) |
Reduces cognitive fatigue and supports learning |
Limitations: However, the Headband Pro cannot access C3/C4/Cz for SMR training. Likewise, Fz remains unavailable for theta up-training. Consequently, central and frontal sites are missing for attention and working memory training.
Dragon EEG
Step 1: QEEG Assessment First (Recommended)
Before any training, perform a QEEG brain map to identify:
- Which brain regions are overactive or underactive during learning tasks
- Specific asymmetries affecting attention or memory
- Individual brainwave patterns affecting learning efficiency
Step 2: Use QEEG Data to Select Your Protocol
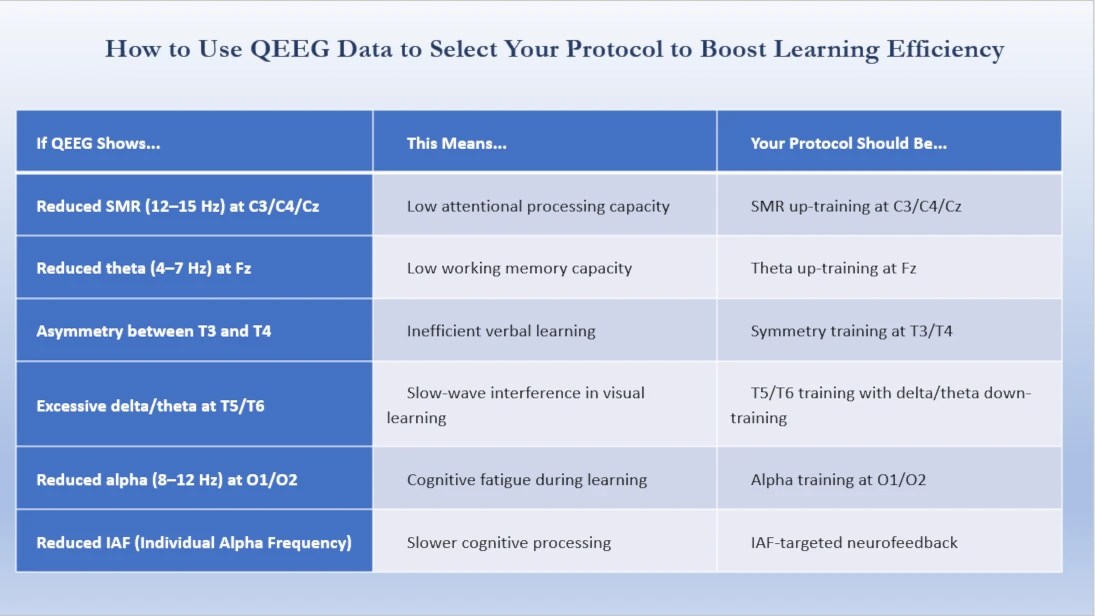
Step 3: Comprehensive Multi-Region Training
With 21 channels, Dragon EEG can train all learning functions simultaneously:
- Attention (SMR at C3/C4/Cz)
- Working memory (Theta at Fz)
- Verbal learning (T3/T4 asymmetry)
- Visual learning (T5/T6)
- Relaxation (Alpha at O1/O2)
All in the same session.
Step 4: Track Progress
Use Dragon EEG’s QEEG capabilities to:
- Monitor changes in learning-related brain activity over time
- Adjust protocols based on objective data
- Generate reports showing learning efficiency improvements
Frequently Asked Questions
Some people notice subtle shifts within the first few sessions—for example, better sleep, reduced mental fog, or improved focus during tasks. However, neurofeedback is a gradual learning process. In most cases, individuals begin to observe more consistent changes after 5–8 sessions. Furthermore, lasting structural changes in cognitive performance typically require 20–40 sessions over several weeks or months. Above all, consistency matters more than session duration.
Most practitioners recommend 1–3 sessions per week initially. Additionally, a typical course involves 20–40 sessions, though this varies depending on individual goals and your brain’s response. Sessions usually last 30–60 minutes. Since the brain learns through repetition, consistency remains essential for lasting results.
No. BrainBit devices are non-medical neurofeedback tools designed for wellness, cognitive performance, and self-regulation. However, they do not diagnose or treat medical conditions. Therefore, always consult a healthcare professional for medical concerns.
Yes. Neurofeedback is particularly effective for children with attention difficulties, learning disabilities, and ADHD. In fact, studies demonstrate that neurofeedback can improve focus, impulse control, and emotional regulation in children with ADHD. Moreover, MINDO is specifically designed with adjustable sizing and app-guided sessions for both adults and children.
Neurofeedback is a non-invasive, low-risk process. Specifically, sensors only read brain activity—nothing enters the brain. Side effects are uncommon. However, some people may experience temporary fatigue, a mild headache, or changes in sleep as the brain adjusts to new patterns. Nevertheless, these effects typically level out quickly.
References
- Zhou, W., Nan, W., Xiong, K. et al. Alpha neurofeedback training improves visual working memory in healthy individuals. npj Sci. Learn. 9, 32 (2024). https://doi.org/10.1038/s41539-024-00242-w
- Liu Z, Jiang Y, Cerel-Suhl S, Zhao X. Neurofeedback-Enhanced Working Memory Training: A Proof-of-Concept for Reversing Age-Related Neural Slowing in Older Adults. medRxiv [Preprint]. 2025 Oct 13:2025.10.08.24316788. doi: 10.1101/2025.10.08.24316788. – https://pubmed.ncbi.nlm.nih.gov/41282693/
- Wang JR, Hsieh S. Neurofeedback training improves attention and working memory performance. Clin Neurophysiol. 2013 Dec;124(12):2406-20. doi: 10.1016/j.clinph.2013.05.020. – https://pubmed.ncbi.nlm.nih.gov/23827814/
- Hsueh JJ, Chen TS, Chen JJ, Shaw FZ. Neurofeedback training of EEG alpha rhythm enhances episodic and semantic long-term memory performance. Sci Rep. 2021 Aug 26;11(1):17274. doi: 10.1038/s41598-021-96726-5. – https://pmc.ncbi.nlm.nih.gov/articles/PMC8390655/
- Vernon D, Egner T, Cooper N, Compton T, Neilands C, Sheri A, et al. The effect of training distinct neurofeedback protocols on aspects of cognitive performance. Int J Psychophysiol. 2003 Jan;47(1):75-85. doi: 10.1016/S0167-8760(02)00091-0. – https://pubmed.ncbi.nlm.nih.gov/12543448/
- Reiner M, Rozengurt R, Barnea A. Better than sleep: theta neurofeedback training accelerates memory consolidation. Biol Psychol. 2014 Jan;95:45-53. doi: 10.1016/j.biopsycho.2013.10.010. – https://pubmed.ncbi.nlm.nih.gov/24211625/
- Eschmann KCJ, Bader R, Mecklinger A. Theta/beta neurofeedback training improves episodic and semantic long-term memory performance. Sci Rep. 2021 Aug 26;11(1):17274. doi: 10.1038/s41598-021-96726-5. – https://pmc.ncbi.nlm.nih.gov/articles/PMC8390655/
- Wang J, Wang J, Chen J, Yao L. Individual alpha neurofeedback training effect on short-term memory. Int J Psychophysiol. 2012 Oct;86(1):83-7. doi: 10.1016/j.ijpsycho.2012.07.182. – https://www.sciencedirect.com/science/article/abs/pii/S0167876012005478
- Monastra VJ, Lynn S, Linden M, Lubar JF, Gruzelier J, LaVaque TJ. Electroencephalographic biofeedback in the treatment of attention-deficit/hyperactivity disorder. Appl Psychophysiol Biofeedback. 2005;30(2):95-114. doi:10.1007/s10484-005-4305-x – https://pubmed.ncbi.nlm.nih.gov/16013783/
- Yeh WH, Ju YJ, Shaw FZ, Liu YT. Comparative effectiveness of electroencephalogram-neurofeedback training of 3-45 frequency band on memory in healthy population: a network meta-analysis with systematic literature search. J Neuroeng Rehabil. 2025;22(1):94. doi:10.1186/s12984-025-01634-8 – https://pubmed.ncbi.nlm.nih.gov/40275307/
- Othmer S, Othmer SF, Kaiser DA. Clinical neurofeedback: case studies and protocols. In: Evans JR, editor. Handbook of Neurofeedback: Dynamics and Clinical Applications. Binghamton, NY: Haworth Medical Press; 2007. Chapter 8. https://social.hse.ru/data/2011/07/12/1214273534/Handbook_NFB2.pdf
BrainBit Family for Cognitive Performance Improvement





At-a-Glance BrainBit Device Selection Matrix
Review the comprehensive protocol maps, anatomical targets, and hardware limitations for each device in the BrainBit family below to choose the perfect headband for your cognitive training goals.
1. MINDO / Headband Protocol Map
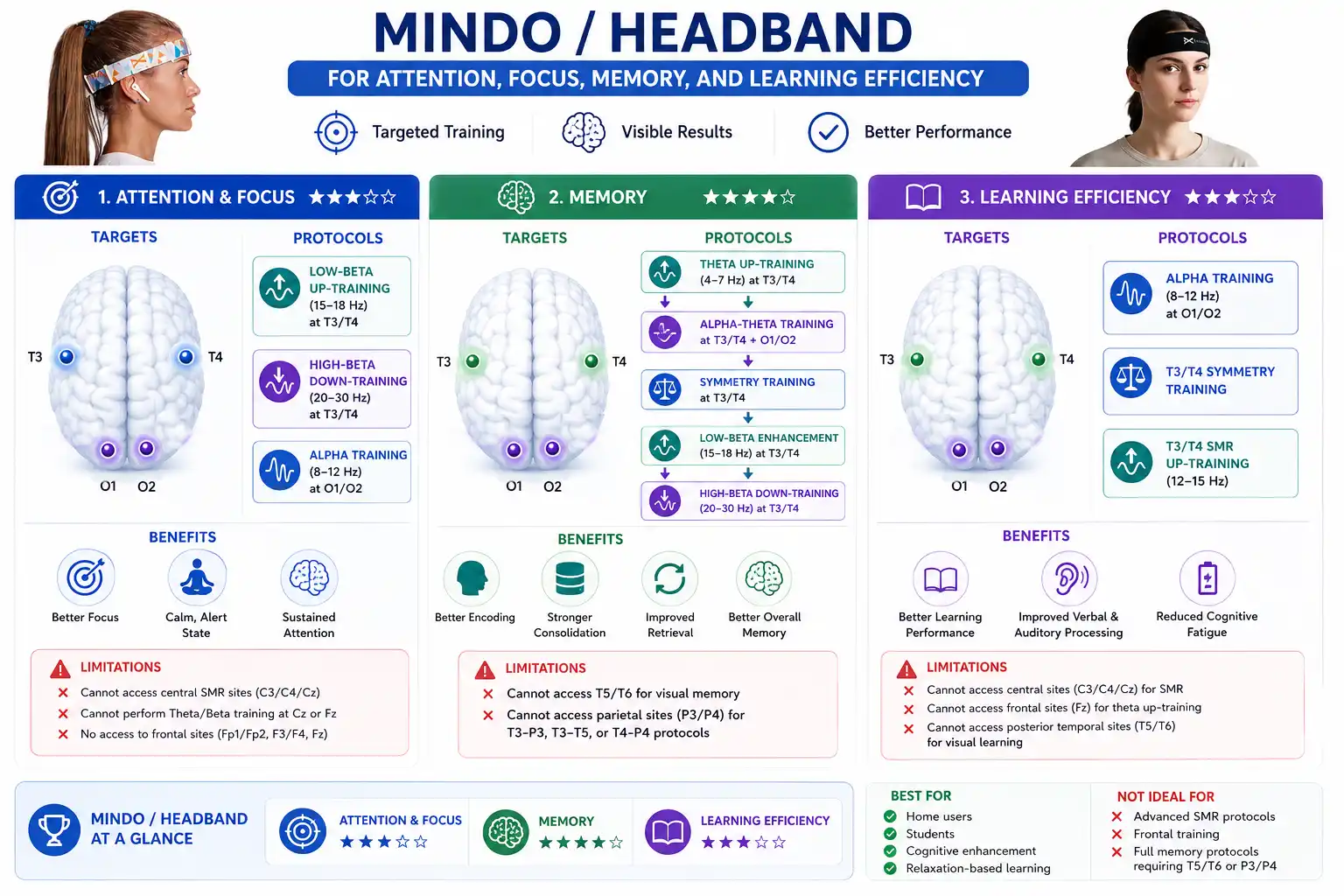
MINDO Quick Verdict: Ideal for home users and students focusing on temporal and occipital training (verbal memory, alpha relaxation, and basic focus). However, it is not ideal for advanced SMR training, frontal protocols, or full memory mapping due to its fixed 4-channel layout.
2. BrainBit Flex 4 Protocol Map
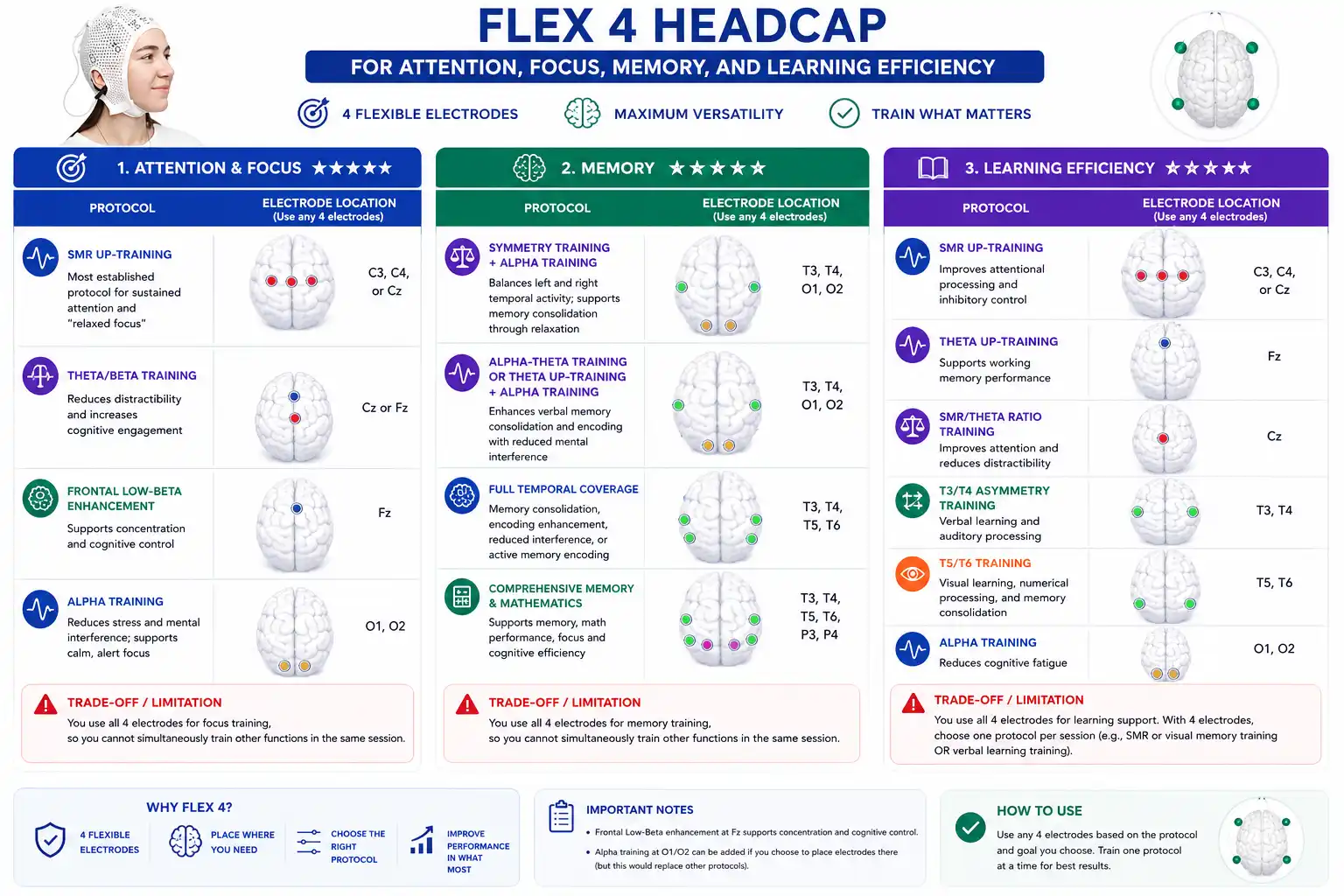
Flex 4 Quick Verdict: Ideal for users seeking maximum versatility and targeted, single-session training goals. With 4 moveable electrodes, it allows you to customize setups for Attention (C3, C4, Cz, Fz), Memory (T3, T4, O1, O2, T5, T6, P3, P4), or Learning Efficiency. However, because you must use all 4 electrodes for a single training target, it is not ideal for users who want to run multiple distinct protocols simultaneously or train different cognitive functions in the same session.